In Part 1 of our ‘Upper Limb Nerve Lesions’ series we learnt about the brachial plexus and the two most commonly occurring lesions associated with damage to it. We now move on to the radial nerve and its associated nerve lesions.
The radial nerve is a major branch of the brachial plexus that arises as a continuation of the posterior cord. It contains nerve fibres from all 5 roots of the brachial plexus (C5 – T1). It supplies the triceps brachii muscle, most of the extensor muscles of the forearm and innervates most of the skin of the posterior aspect of the forearm, the lateral side of the palm and the lateral three and a half fingers.
Anatomy of the Radial Nerve
The radial nerve arises in the axilla and initially descends posterior to the axillary and brachial arteries. It then passes inferior to the tendons of latissimus dorsi and teres major to run with the profunda brachii artery between the long and medial heads of triceps before passing through the lateral triangular space. Before leaving the axilla it supplies the medial head of triceps and gives off the posterior cutaneous nerve of the arm.
It then travels through the spiral groove of the humerus between the lateral and medial heads of triceps giving off the following branches whilst in the groove:
- Branch to the medial head of triceps
- Inferior lateral cutaneous nerve of the arm
- Posterior cutaneous nerve of the forearm
The radial nerve then emerges from the spiral groove on the lateral aspect of the humerus, pierces the lateral intermuscular septum at the mid point of the humerus and enters the anterior compartment of the arm. It then passes inferiorly between brachialis and brachioradialis before entering the lateral cubital fossa. It then passes anteriorly to the lateral epicondyle and continues into the forearm. Within the forearm the nerve terminates by dividing into two branches:
- The deep branch of the radial nerve and;
- The superficial branch of the radial nerve
The deep branch of the radial nerve is a primarily motor branch. It pierces the supinator muscle, winds around the radius to reach the posterior forearm and then pierces the supinator again. Once in the posterior forearm it becomes known as the posterior interosseous nerve (PIN). In 30% of people it passes through a fibrotendinous structire below the supinator muscle called the arcade of Frohse. The PIN supplies all of the extrinsic wrist extensors except for extensor carpi radialis longus.
The superficial branch of the radial nerve is a primarily sensory branch. It descends into the forearm under brachioradialis running with radial artery on its medial aspect from 1/3 of the way down the forearm. It passes posteriorly, emerging from under the tendon of brachioradialis proximal to the radial styloid and passes over the tendons of the anatomical snuffbox. It then terminates as cutaneous branches to the dorsum of the hand.
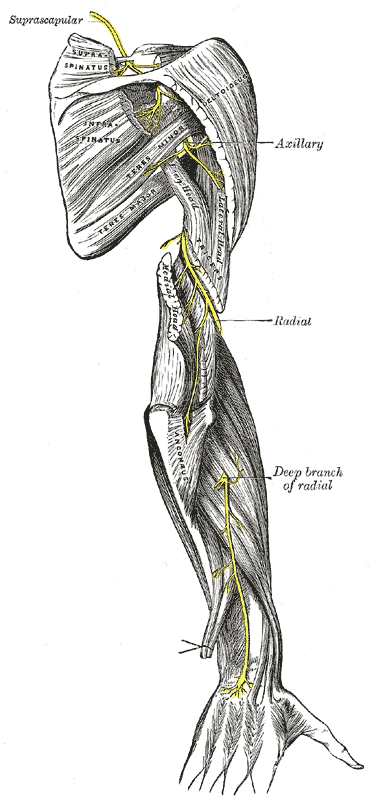
Fig 1. The course of the radial nerve (from Gray’s Anatomy).
The Motor Function of the Radial Nerve
The muscles supplied by the radial nerve and its two main motor branches are shown in the table below:
| Branch | Muscles supplied |
|---|---|
| The radial nerve | Medial head of triceps brachii Lateral head of triceps brachii Anconeous Brachioradialis Extensor carpi radialis longus |
| The deep branch of the radial nerve | Extensor carpi radialis brevis Supinator |
| The posterior interosseous nerve | Extensor digitorum Extensor digiti minimi Extensor carpi ulnaris Abductor pollicis longus Extensor pollicis brevis Extensor pollicis longus Extensor indicis |
The Sensory Function of the Radial Nerve
The sensory function of the radial nerve is provided by its four main sensory branches:
- Inferior lateral cutaneous nerve of the arm – supplies the lateral aspect of the anterior upper arm between the deltoid and the elbow
- Posterior cutaneous nerve of the arm – supplies part of the posterior aspect of the upper arm
- The posterior cutaneous nerve of the forearm – supplies a tapered strip of the middle portion of the posterior forearm
- The superficial branch of the radial nerve – supplies the posterior surface of the lateral 3 ½ digits and the associated areas of the palm
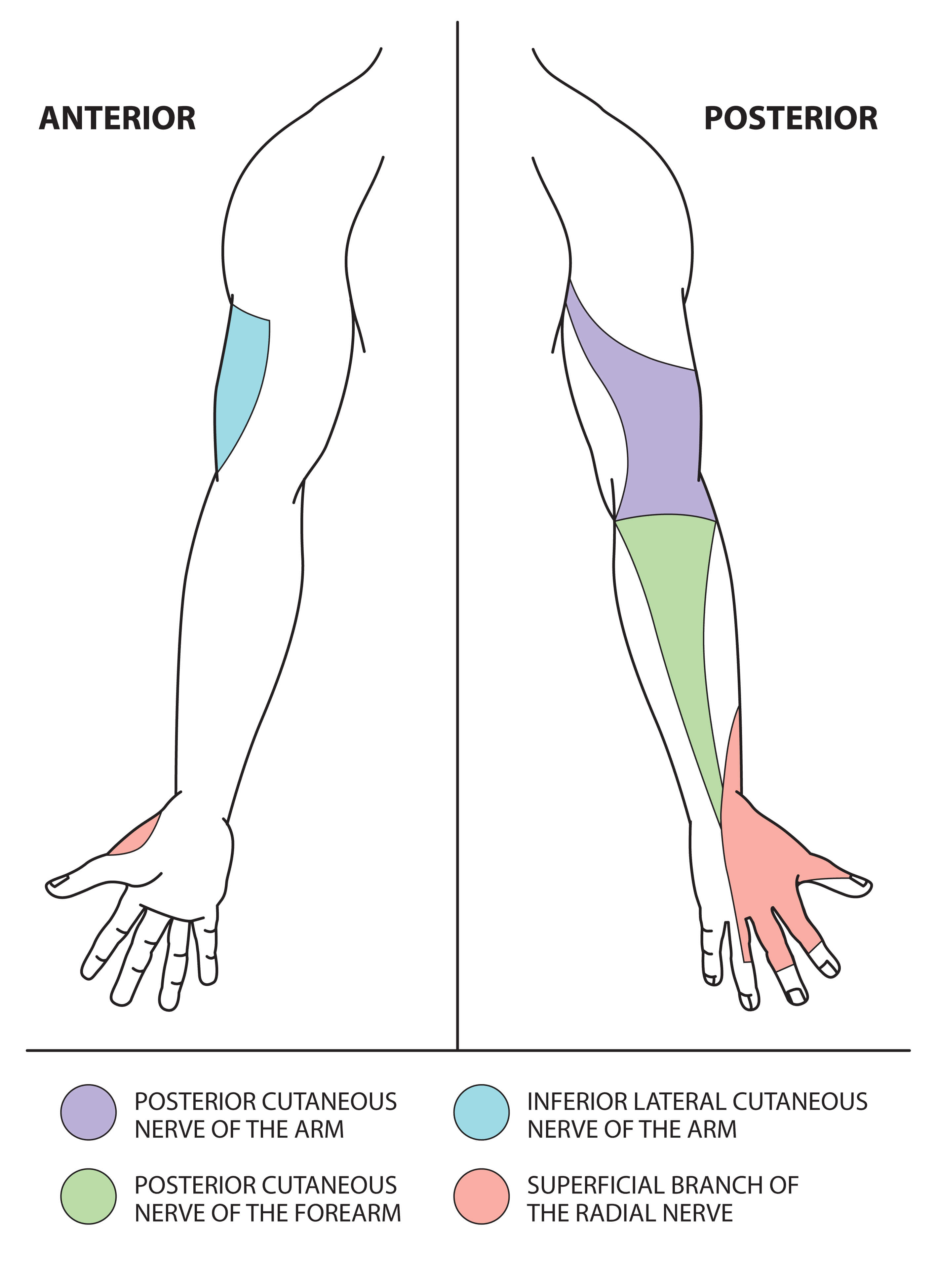
Fig 2. The sensory function of the radial nerve. © Medical Exam Prep
Radial Nerve Lesions in the Axilla
The radial nerve can be damaged in the axilla by glenohumeral joint dislocation or fracture of the head of the humerus. It can also occur due to excessive pressure in the axilla, for example ‘Saturday night syndrome’ where the arm has been hung over the back of a chair in a drunken stupor.
Motor damage:
All of the muscles innervated by the radial nerve will be paralysed including triceps brachii and brachioradialis. There will be loss of elbow extension. The patient will also be unable to extend the forearm, wrist and fingers and wrist drop will be evident.
Sensory damage:
All four cutaneous branches of the radial nerve will be affected and there is loss of sensation over the lateral and posterior upper arm, posterior forearm and the posterior surface of the lateral 3 ½ digits and the associated areas of the palm.
Radial nerve Lesions in the Spiral Groove
The commonest cause of a radial nerve palsy is external compression or trauma to the radial nerve as it traverses the spiral groove in the mid-humerus. Injuries here are commonly associated with fractures of the humerus.
Motor damage:
The triceps and brachioradialis are often spared when there is injury in the spiral groove and elbow extension is spared. The deep branch of the radial nerve is affected and the muscles in the posterior forearm compartment are paralysed. The patient will be unable to extend the forearm, wrist and fingers and wrist drop will be evident.
Sensory damage:
The posterior cutaneous nerve of the arm arises in the axilla and will be spared. The inferior lateral cutaneous nerve of the arm and posterior cutaneous nerve of the forearm often arise in the spiral groove and may also be spared. There is loss of sensation over the posterior surface of the lateral 3 ½ digits and the associated areas of the palm.
Radial Nerve Lesions at the Elbow
The deep branch of the radial nerve can be damaged in isolation at the elbow by fracture of the radial head or by posterior dislocation of the elbow.
Motor damage:
If the deep branch of the radial nerve is damaged the muscles of the posterior compartment of the forearm will be paralysed, apart from extensor carpi radialis longus, which is supplied higher up the arm. Because the extensor carpi radialis longus is a strong extensor wrist drop will not occur but there will be weakness of wrist extension.
Sensory damage:
The deep branch of the radial nerve is a purely motor nerve and if damaged in isolation there will be no associated sensory loss.
Radial Nerve Lesions in the Forearm
Stabbing or laceration of the forearm, particularly in the region of brachioradialis, can result in isolated damage to the superficial branch of the radial nerve.
Motor damage:
As the superficial branch of the radial nerve is a sensory branch there is no associated motor loss.
Sensory damage:
There is loss of sensation over the posterior surface of the lateral 3 ½ digits and the associated areas of the palm.
Injury to the Posterior Interosseous Nerve in the Forearm
The posterior interosseous branch of the radial nerve may also be damaged in the forearm, either by an injury to the radial head or by becoming entrapped in the supinator muscle under the arcade of Frohse.
Motor damage:
Paralysis is similar to damage to the deep branch of the radial nerve but extensor carpi radialis brevis and supinator are also spared.
Sensory damage:
The posterior interosseous nerve is a purely motor nerve and if damaged in isolation there will be no associated sensory loss.
Next: Upper Limb Nerve Lesions Part 3 – The Median Nerve
Thank you to the joint editorial team of www.anatomyprep.co.uk for this ‘Exam Tips’ blog post.
Header image used on licence from Shutterstock




I am an ODP currently studying an advanced role as a surgical first assistant. This sight has been excellent for advancing my knowledge and helping with the written criteria for the course. Good clear diagrams provided and a clear, easy to understand explanation provided.
Thank you.