Digital clubbing is one of the oldest recognised signs in medicine, first formally documented by Hippocrates nearly 2500 years ago. For this reason, it is also known as “Hippocratic fingers”.
It is an important clinical sign that can assist in the diagnosis of a variety of conditions, particularly when found in conjunction with other symptoms and signs. Digital clubbing is characterised by a painless and bilateral increase in the soft tissue around the end of the fingers and toes.
Pathogenesis
The exact mechanism behind digital clubbing remains unclear, but it is thought to involve increased interstitial fluid volume and enhanced blood flow to the digits. Platelet-derived growth factor and vascular endothelial growth factor are believed to play key roles in this process.
Aetiology
Digital clubbing is associated with a wide variety of clinical condition. The commonest causes lung diseases, with neoplastic lung disease being the most common respiratory cause of clubbing.
The following table summarises the most common causes:
| System involved | Examples |
|---|---|
| Primary clubbing | Primary hypertrophic osteoarthropathy (pachydermoperiostosis) Genetic (familial clubbing) Hypertrophic osteoarthropathy |
| Cardiac disease | Cyanotic congenital heart disease Bacterial endocarditis |
| Respiratory disease | Lung cancer Tuberculosis Bronchiectasis Cystic fibrosis Interstitial lung disease Cryptogenic fibrosing alveolitis Idiopathic pulmonary fibrosis Sarcoidosis Empyema Pleural mesothelioma Pulmonary metastases |
| Gastrointestinal disease | Ulcerative colitis Crohn's disease Primary biliary cirrhosis Cirrhosis of the liver Oesophageal achalasia Peptic ulceration |
| Endocrine disease | Acromegaly Thyroid acropachy |
| Dermatological disease | Bureau-Barrière-Thomas syndrome Fischer's syndrome Palmoplantar keratoderma |
| Malignancy | Thyroid cancer Thymus cancer Hodgkin disease Disseminated chronic myeloid leukaemia |
Clinical presentation
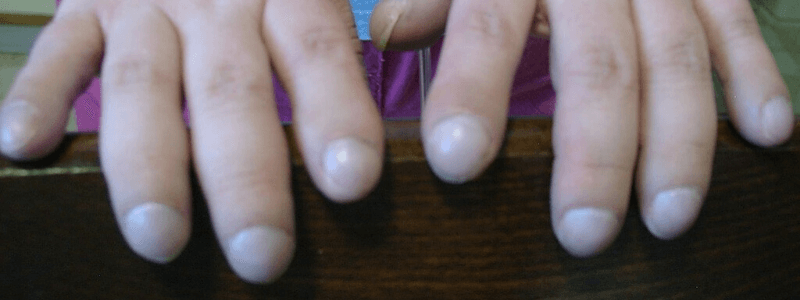
There is typically bilateral swelling of the distal portion of the fingers or toes. The onset is slow and may go unnoticed by the patient. Digital clubbing is generally painless, but some patients report mild discomfort. It is most commonly discovered as part of an examination for other presenting symptoms.

Prominent digital clubbing Wikipedia
Courtesy of Desherinka CC BY-SA 4.0
As clubbing progresses, the Lovibond angle—the angle between the nail and the nail base—becomes lost. Normally, this angle is ≤160°, but as the nail becomes more convex, it increases to >180°. In early clubbing, the nail may feel spongy on palpation, and the skin at the base may appear smooth and shiny.
In people without clubbing, placing the dorsal surfaces of two opposing fingers together creates a small, diamond-shaped gap between the nail beds. When clubbing is present, this gap disappears and the angle between the nails widens. This is known as Schamroth’s window test.
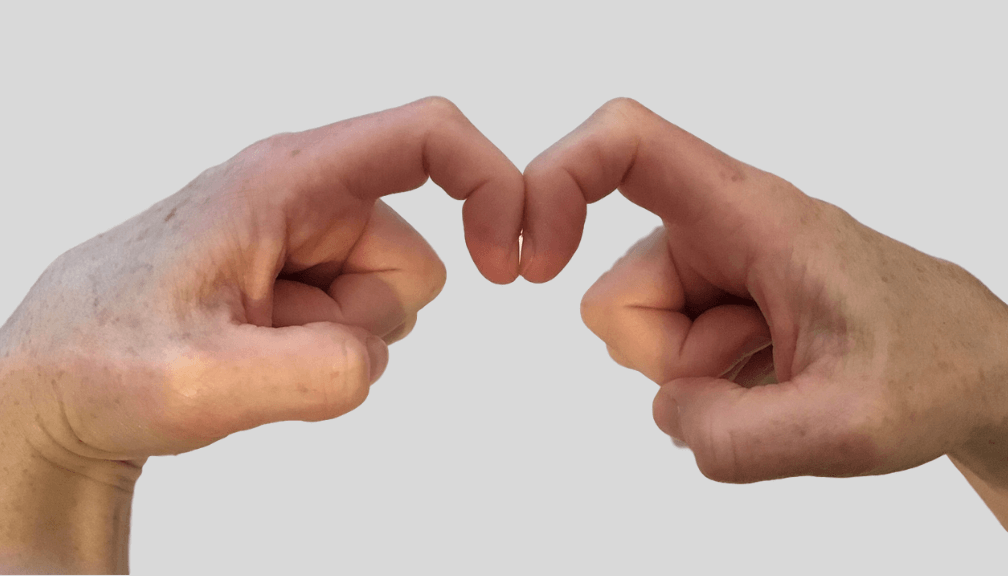
A normal Samoroth’s window test in a patient without digital clubbing
Grading
Digital clubbing is graded as follows:
| Grade | Description |
|---|---|
| Grade 1 | Fluctuation or softening of the nail bed |
| Grade 2 | Increase in the Lovibond angle to greater than 160° |
| Grade 3 | Accentuated convexity of the nail |
| Grade 4 | Clubbed appearance of the fingertip |
| Grade 5 | Development of a shiny or glossy change in the nail and adjacent skin with longitudinal striations |
Thank you to the joint editorial team of www.plabprep.co.uk for this ‘Exam Tips’ post.




