
A 22-year-old athlete presents with a history of palpitations that have been occurring whilst he is playing football. They have become bothersome of late and his coach has advised him to have a medical check up. On questioning him you find out that his father died at a young age of an unknown cause. On examination his pulse feels ‘jerky’ and you can palpate a double apical impulse. He has an ejection systolic murmur at the left sternal edge that radiates throughout the praecordium.
1. What is the most likely diagnosis?
Show Answer
This patient has hypertrophic obstructive cardiomyopathy (HOCM). HOCM is a primary disease of the heart in which the left and right ventricles are hypertrophied. It is the commonest cause of sudden cardiac death in young people and athletes. HOCM affected approximately 1 in 500 people worldwide and the annual mortality is estimated to be in the region of 1-2%.
2. Is this disease an inherited disorder?
Show Answer
HOCM is a heterogenous disorder, produced my mutations in multiple genes coding for sarcomeric proteins, for example the beta-myosin heavy gene and troponin T. The inheritance is primarily autosomal dominant but penetrance is variable. Over 150 different mutations have now been indentified and the clinical phenotype is highly variable.
3. What other symptoms and signs might you expect to be present?
Show Answer
A wide variety of clinical symptoms and signs can be seen in HOCM. Often the diagnosis is coincidental in asymptomatic patients.
Symptoms present in HOCM include:
- Palpitations
- Breathlessness
- Chest pain
- Syncope
Clinical signs present in HOCM include:
- Jerky pulse character
- Double apical impulse (palpable atrial and ventricular contraction)
- Thrill at left sternal edge
- Ejection systolic murmur at the left sternal edge that radiates throughout the praecordium
- 4th heart sound may be present due to blood hitting a hypertrophied stiff left ventricle during atrial systole
4. What would you expect to find on an ECG in this case?
Show Answer
Most patients with HOCM have an abnormal ECG but ECG findings do not correlate with the clinical outcome.
Typical ECG findings include:
- Left ventricular hypertrophy
- Non-specific T wave and St segment changes
- Deep, narrow ‘dagger-like’ Q waves (caused by asymmetrical septal hypertrophy)
- Left atrial hypertrophy and ‘P mitrale’
In addition there is an association between HOCM and Wolff-Parkinson-White (WPW) syndrome and atrial fibrillation and SVTs are also commonly seen.
ECG demonstrating ‘dagger-like’ Q waves:
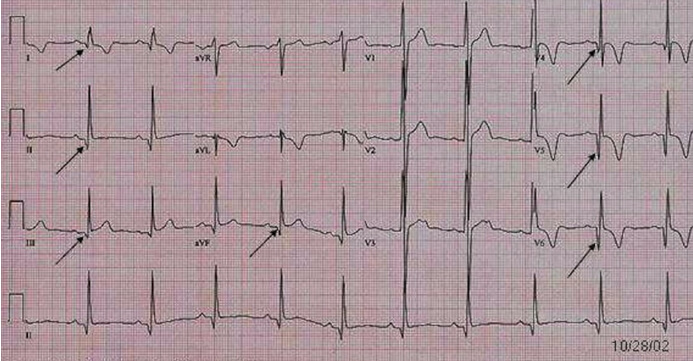
This ECG was sourced from www.lifeinthefastlane.com:
5. How is this condition managed?
Show Answer
An expert cardiologiocal opinion is essential for the management of this highly variable and complex condition.
Patients presenting with angina and breathlessness can often be successfully treated with the administration of beta-blockers. Arrhythmias are common and can sometimes be treated medically with drugs, such as amiodarone, but in many cases catheter ablation is required. Atrial fibrillation in patients with HOCM is associated with a high risk of thromboembolism and these patients should be anticoagulated.
If outflow obstruction is present, negatively inotropic drugs, such as verapamil, beta-blockers and disopyramide, can be used with varying degrees of success. Patients with refractory symptoms can be considered for surgical intervention with myomectomy.
Above all patients should be made aware of the risk of sudden death and many patients receive an implantable cardioverter defibrillator (ICD).




Good questions
Good Question