Pneumonia, which is defined as inflammation of the lung, is a common cause of morbidity and mortality around the world. Every year between 0.5% and 1% of adults in the U.K. will develop community-acquired pneumonia.
Pneumonia is characterised by exudation and consolidation into the alveoli, and in the U.K. Streptococcus pneumoniae is by far the most common causative organism. Chest X-rays are the initial modality of investigation in the majority of cases, and a sound understanding of the chest X-ray features of pneumonia is vital for all front-line clinicians that encounter and treat it.
How can shadow puppets help us to understand chest X-rays?
The silhouette sign refers to the loss of normal borders between thoracic structures on a chest X-ray. It is something of a misnomer as it actually represents the loss of a normal silhouette. Much is made of this sign in radiology and, once it is properly understood, it is extremely useful in localising areas of airspace opacity, atelectasis, or a mass within the lung. Loss of these normal silhouettes on an AP chest X-ray is generally indicative of the site of the pathology.
This sign can be difficult to conceptualise, but the simple children’s game of hand shadow puppets is a helpful way of assisting our understanding of it. The game works because you cannot tell where one hand begins and the other ends. The combination of their individual silhouettes adds up to become a bird, a rabbit, a dog and all manner of other possibilities.

Shadow of two hands forming the shape of a bird, image sourced from Wikipedia
Courtesy of Hedgehog83 CC BY-SA 3.0
If we apply this to a chest X-ray, it becomes evident that the only structures we can appreciate are those where there is a density change at their border with neighbouring structures. X-rays travelling through lung tissue cast less of a shadow than those passing through the soft tissues of the mediastinum or abdomen.
Consolidation
In the case of pneumonia, air within the alveoli is replaced by inflammatory exudate and pus. Affected alveoli become as dense as soft tissue structures such as the heart. In the lobes which abut the heart anatomically, it therefore, becomes impossible to distinguish where the lung ends, and the heart begins. The same is true for the hemidiaphragms. This is termed the silhouette sign and is often described as causing a ‘loss of clarity’.
Where the horizontal fissure is concerned, this can sometimes be seen as a sharp border in the mid-zone of the right hemithorax when there is consolidation in the alveoli either above it (in the right upper lobe) or below it (in the right middle lobe).
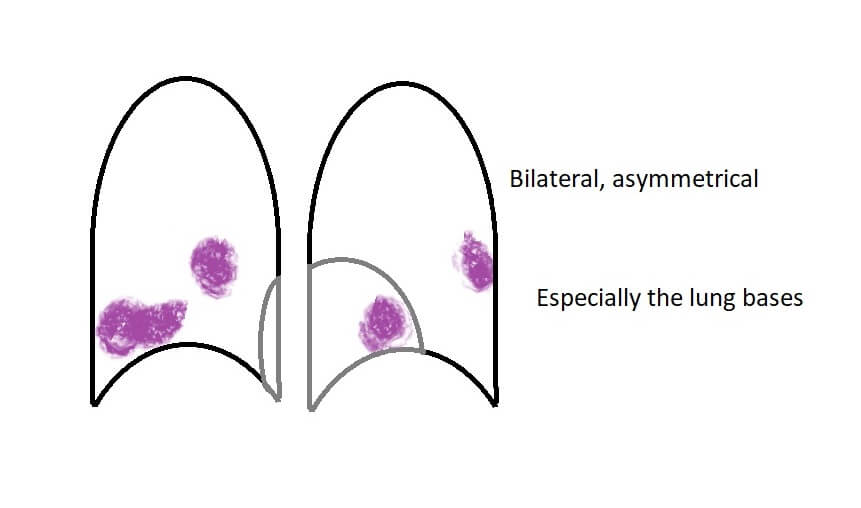
Bronchopneumonia appears on a chest X-ray as bilateral patchy shadows and typically predominates at the lung bases:
Lobar pneumonias have specific appearances, which can be explained by the anatomical relationships of the lobes of the lung to their surrounding structures.
To determine which lobe is affected ask two questions:
- What can I see?
- What can I not see?
What can I see?
| I can see: | Pathology is situated in: |
|---|---|
| Heart borders and hemidiaphragms | Upper lobes |
| Horizontal fissure | Right upper or middle lobe |
What can I not see?
| I can’t see: | Pathology is situated in: |
|---|---|
| Left heart border | Lingula |
| Right heart border | Right middle lobe |
| Left hemidiaphragm | Left lower lobe |
| Right hemidiaphragm | Right lower lobe |
The following illustrated examples should make this even clearer.
Right upper lobe consolidation:
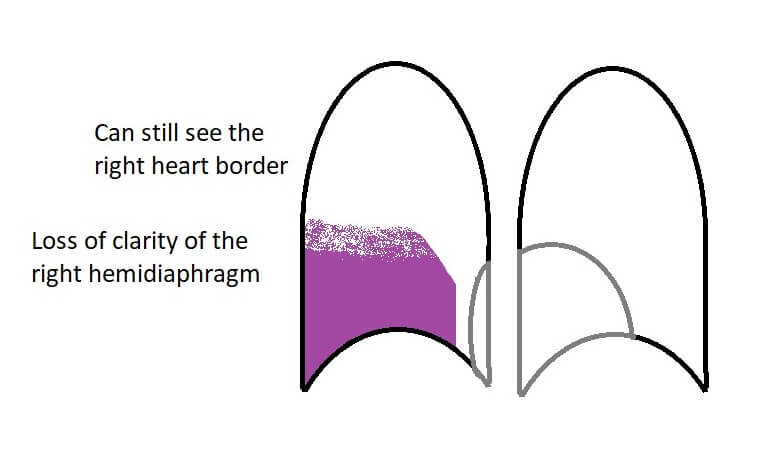
Right middle lobe consolidation:
Right lower lobe consolidation:
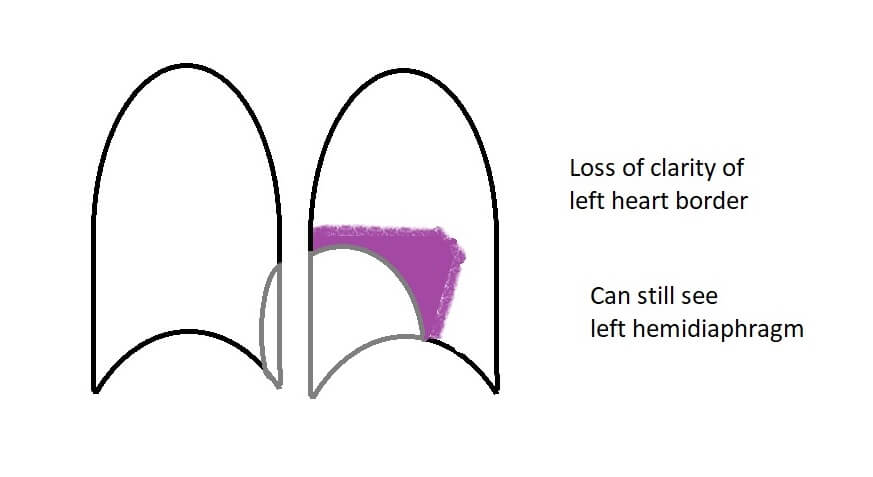
Left upper lobe consolidation:

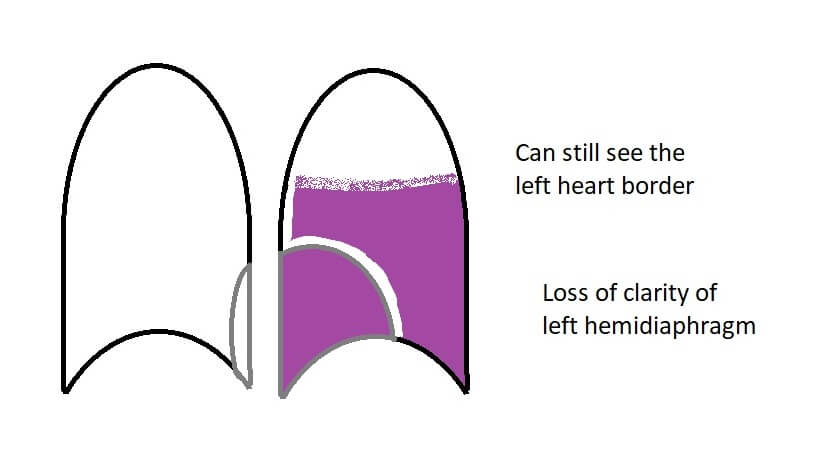
Left lower lobe consolidation:
Lingula consolidation:
Of course, it is not always the case that the entirety of a given lobe is affected in which case only one or part of one aspect of the features described may be discernible.
A round pneumonia is a specific entity encountered in the field of paediatrics. The collateral pores of Kohn allow air drift between adjacent alveoli. It is through these that an infection can spread in adults, but they do not start to form until around 3-4 years of age. Infection in children is thus better contained and can appear as a well-defined, rounded area on a chest x-ray.
Collapse
Lobar collapse can be caused by a number of entities as detailed in the diagram below:
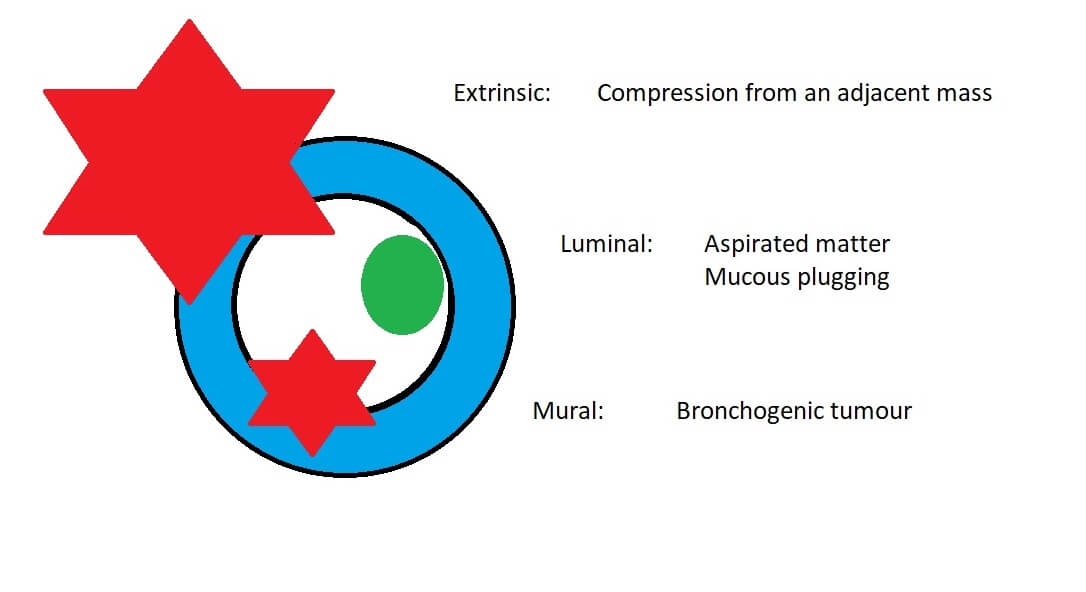
Once the airway is completely occluded, trapped air distal to the obstruction is absorbed into the surrounding tissues collapsing the alveoli as it does so. The collapsed alveoli take up a far smaller volume than aerated lung, i.e. there is volume loss. Volume loss results in the appearance of any or all of a number of key chest X-ray signs. If present, however, they only confirm the presence of collapse and do not give any further information as to the precise location of the collapse within that lung, or the underlying aetiology:
- Elevation of the hemidiaphragm
- Mediastinal shift (towards the pathology)
- Rib crowding
- Bronchovascular crowding
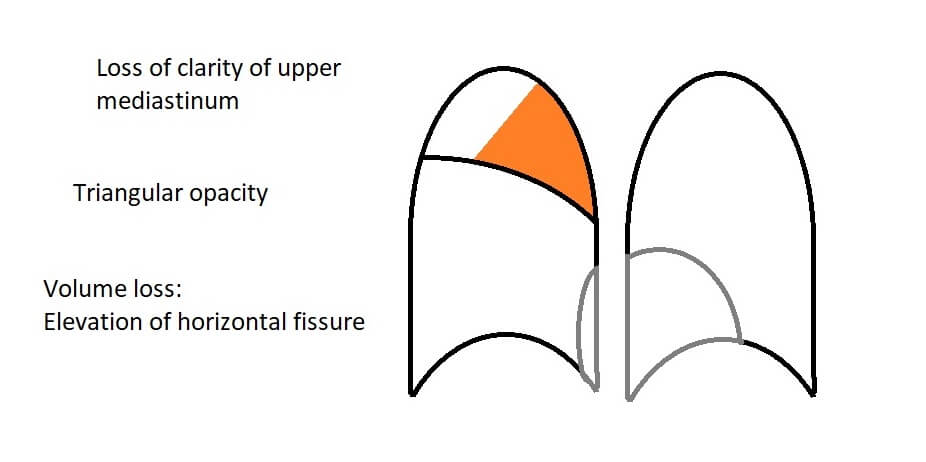
Collapse of each lobe individually gives rise to particular distinct patterns which can be recognised on a chest X-ray. All appear as triangularly shaped opacities in an area pertinent to their anatomy. The exception is a left upper lobe collapse.
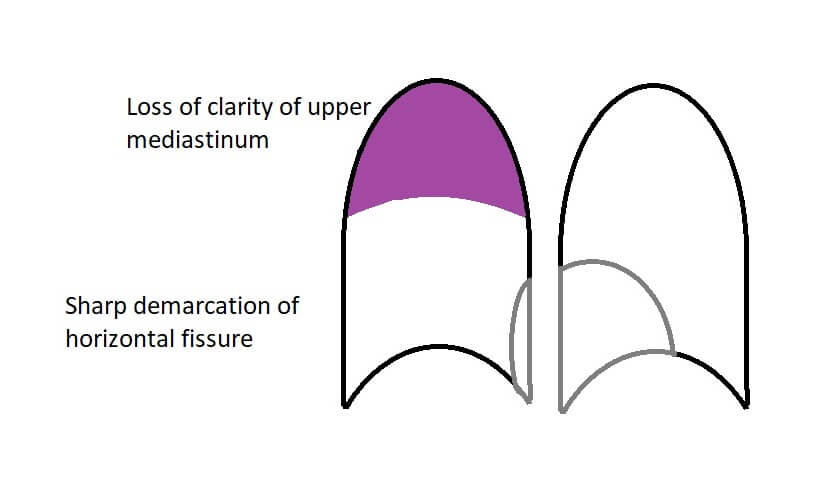
When the right upper lobe collapses, it does so towards the middle of the body. Loss of clarity of the upper mediastinum, is therefore, a consequence. Elevation of the horizontal fissure occurs due to volume loss:
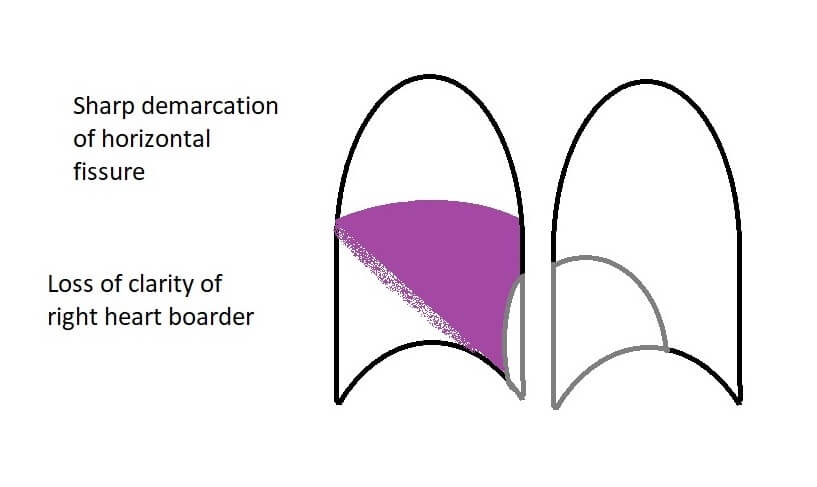
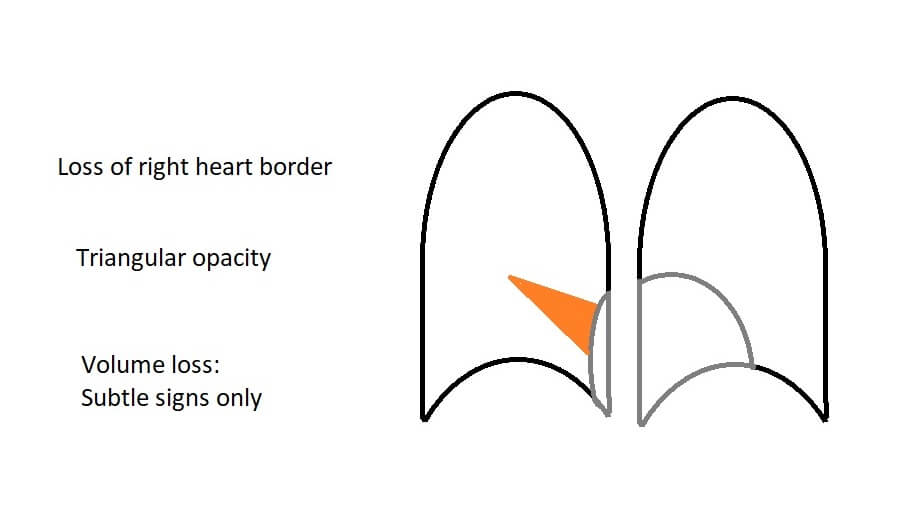
Collapse of the right middle lobe gives minimal evidence of volume loss radiologically. The key sign for middle lobe collapse is loss of clarity of the right heart border:
In right lower lobe collapse the right heart border (which is adjacent to the right middle lobe) is still visible but there will be a triangular opacity at the right cardiophrenic angle:
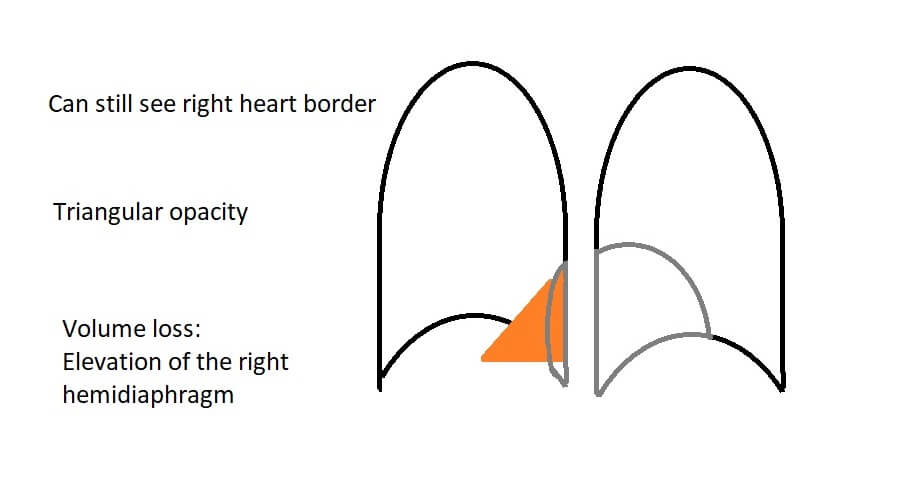
This can be seen more clearly on the example chest X-ray below:
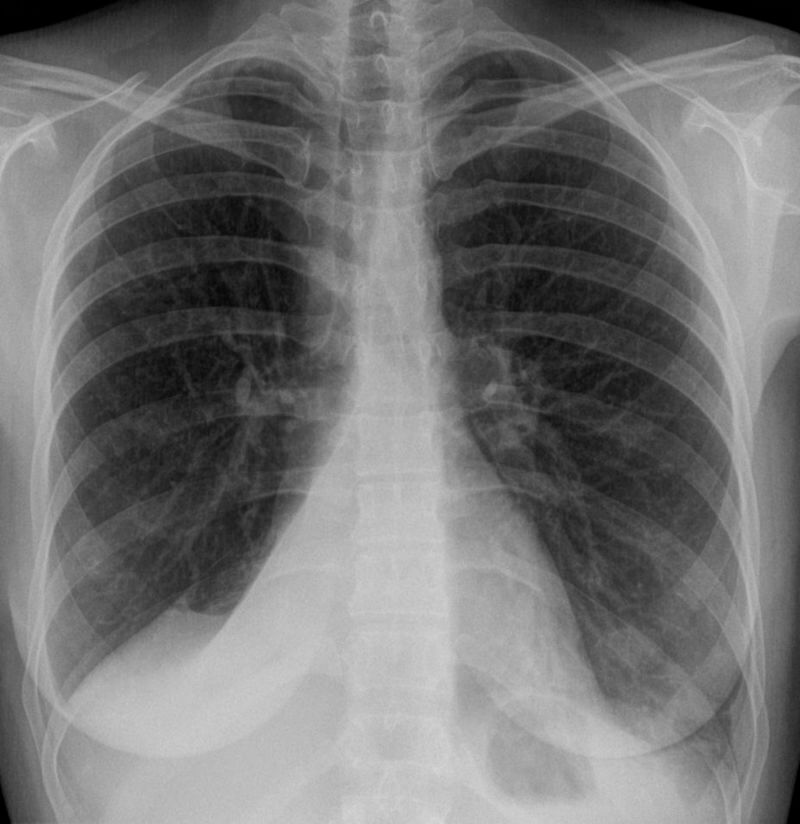
Right lower lobe collapse, X-ray sourced from Wikipedia
Courtesy of Hellerhoff CC BY-SA 3.0
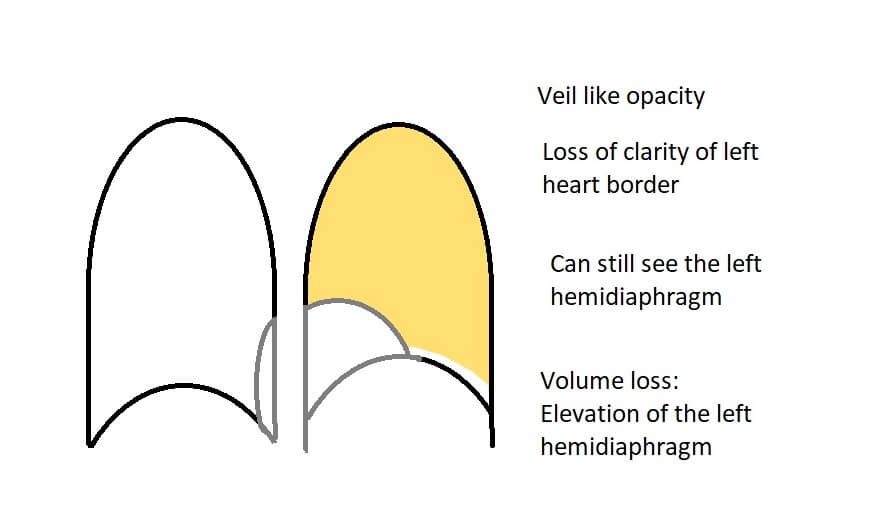
The left upper lobe is large and anteriorly situated. When it collapses, it flattens vertically against the anterior chest wall and consequently is seen as a veil-like opacity covering almost the whole hemithorax. Since the aerated lower lobe is still sitting on the diaphragm, the diaphragm will still be seen very clearly although the left heart border may be obscured:
Collapse of the left lower lobe can give rise to a double left heart border where the triangularly shaped opacity of the collapsed left lower lobe sits behind the heart and creates a second ‘edge’ next to the edge of the heart. In some cases, this does not occur since the two can overlap sufficiently as to be indistinguishable.

The following table summarises these findings:
| Triangular opacity? | Loss of clarity of… | Other features | |
|---|---|---|---|
| Right upper lobe | Yes | Upper mediastinum | Elevation of the horizontal fissure |
| Right middle lobe | Yes | Right heart border | Minimal signs of volume loss |
| Right lower lobe | Yes | Hemidiaphragm | Can still see the right heart border |
| Left upper lobe | NO (veil-like opacity) | Left heart border | Can still see the hemidiaphragm |
| Left lower lobe | Yes | Hemidiaphragm | Double left heart border |
Air trapping
Air trapping occurs when there is intermittent airway occlusion, for example by a small mucous plug acting as a ball-valve mechanism. In air trapping, there isn’t sufficient time for the trapped air to be absorbed before more air enters past the intermittent obstruction.
In summary
Although chest X-ray interpretation can seem intimidating at first, and the determining which lobe is affected can sometimes be challenging, by following these simple principals you should be able to do so with relative ease. We strongly recommend that you take these principals with you into your everyday clinical practice and try them out as often as possible when evaluating your patient’s chest X-rays.
Header image used on licence from Shutterstock
All other images © Medical Exam Prep unless otherwise stated.
Thank you to the joint editorial team of www.frcrexamprep.co.uk for contributing this educational article.




Excellent and easy to understand description.
Very good article, thanks for the tips.
Brilliant!!!
Excellent
Very good article
Thank you