The ingestion of foreign bodies is a common problem that presents frequently to Emergency Departments. Although it can affect any age group, it is most frequently seen in young children between 6 months and 5 years. Coins are the most commonly swallowed objects, but virtually any object small enough to pass through the pharynx can be swallowed.
Most ingested foreign bodies will pass spontaneously. Although at least 80% of foreign objects pass without the need for intervention, some will cause damage to the gastrointestinal tract and/or become lodged.
Clinical assessment
A thorough patient history is fundamental when evaluating a patient who may have swallowed a foreign body. Patients swallowing foreign bodies are usually asymptomatic, but symptoms can result. It is important to understand the nature of the ingested object, the time of ingestion, and any associated symptoms such as pain, difficulty swallowing, or respiratory distress. In rare circumstances, it may even lead to life-threatening obstruction of the upper gastrointestinal and respiratory tracts.
Clinical assessment should include a focused physical examination, emphasising signs of airway compromise, gastrointestinal obstruction, or perforation. Recognition of red flags, such as drooling, stridor, or severe abdominal pain, is crucial for timely intervention.
Investigations
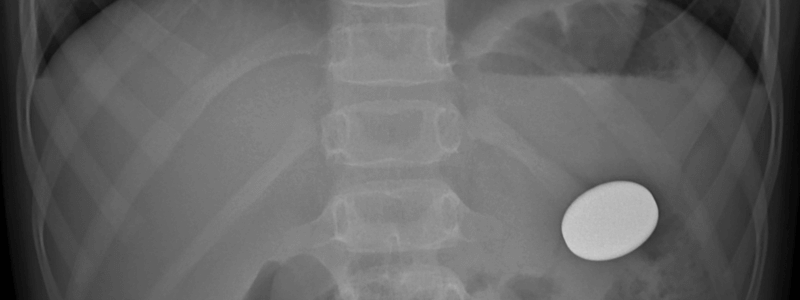
Plain radiographs, including anteroposterior and lateral views of the neck, chest, and abdomen, can aid in identifying the presence and location of radio-opaque foreign bodies.
Metal detectors have been used to detect metal foreign bodies in several studies and have been proven to be both sensitive and specific in confirming the presence of coins in particular and localising them to above or below the diaphragm. They are a helpful adjunct in the assessment of patients who have ingested a foreign body and are recommended in the
Advanced imaging modalities like computed tomography (CT) or endoscopy may be indicated for cases where the foreign body is not visible on initial radiographs or when complications are suspected.
Management
Patients with a history of swallowing a radiolucent foreign body and are asymptomatic with normal examination can be reassured and discharged with advice to return if any significant symptoms appear.
Patients who have a history of swallowing a radiolucent foreign body and are symptomatic, for example, drooling, foreign body sensation, chest pain, dysphagia or swallowing difficulty, should be referred to either the ENT or general surgical teams, depending upon local guidelines.
If a radio-opaque metallic object has been swallowed, it should be possible to assess whether or not the object has passed into the stomach. Good evidence exists for localising coins with a metal detector, if one is available. For non-coin metal objects or when a metal detector is not available, conformation with a chest X-ray is recommended in most guidelines.
An object causing total oesophageal obstruction requires removal under anaesthesia. When an object is causing partial obstruction, and the patient can swallow saliva successfully, it generally has a good chance of passing. Under these circumstances, the patient may be observed for a few hours. If it does not pass, it will need to be removed. If food is thought to have impacted in the lower oesophagus, small amounts of fizzy cola drink may help move it.
Once the object is in the stomach, it will almost certainly pass spontaneously. Inform the patient or parents to return immediately if there is abdominal pain, vomiting, haematemesis or malaena.
There is no place for arranging follow-up visits, repeat X-rays or parental faecal examinations. This does not apply to the ingestion of lead foreign bodies, which can cause systemic lead absorption if they are retained for more than a few days.
Sharp objects should be treated in the same way as other metal foreign bodies, but it should be noted that complication rates increase from less than 1% to 15 to 30%
Beware of ingested magnets. If two or more magnets are swallowed, the attractive force between them can result in local damage to the intestinal wall. Consider endoscopic removal if they are in the stomach. If they have passed beyond the stomach, then close follow-up and early surgical intervention are indicated if the patient becomes symptomatic.
Management summary
The following flow chart outlines the management of ingested foreign bodies in the Emergency Department:

Header image used on licence from Shutterstock.
Thank you to the joint editorial team of www.mrcemexamprep.net for this article.




