Pregnancy, also referred to as gestation, is the period during which one or more offspring develop inside the uterus. It typically lasts around 40 weeks from the first day of the last menstrual period (LMP) and is divided into three trimesters. The first trimester spans from 0 to 12 weeks, the second from 12 to 28 weeks, and the third from 28 weeks until delivery. A delivery before 37 weeks is classified as preterm, while delivery after 42 weeks is considered post-term.
Gestational age describes how far along the pregnancy is, measured in weeks from the LMP to the present. The estimated date of delivery (EDD) is commonly calculated using Naegele’s rule, which adds one year, subtracts three months, and adds seven days to the date of the LMP.
Fertilisation and Blastocyst Formation
After fertilisation, the zygote undergoes a series of mitotic divisions, beginning with two blastomeres. By the third day, continued division results in a 16-cell stage known as the morula, which is a solid ball of cells encased in the zona pellucida. Once the morula enters the uterine cavity, fluid begins to accumulate between its cells, forming the blastocyst by day four.
The early blastocyst consists of two main structures: the inner cell mass, which will become the embryo, and the trophectoderm, which gives rise to the trophoblast. Around two days later, the blastocyst sheds the zona pellucida in a process known as embryo hatching, aided by proteases from the uterine endometrial glands. At this point, the embryo begins absorbing nutrients from uterine secretions in preparation for implantation.
Implantation
Implantation usually occurs between six and seven days post-fertilisation and is mediated by both hormonal signals (primarily oestrogen and progesterone from the corpus luteum) and cell surface interactions between the blastocyst and endometrium. This process unfolds in three distinct phases.
In the apposition phase, the blastocyst loosely aligns itself with the endometrium, typically on the upper posterior uterine wall. This is followed by adhesion, during which the physical contact between the blastocyst and endometrium strengthens. Finally, in the invasion phase, the blastocyst penetrates into the endometrial lining, the upper third of the myometrium, and the maternal vasculature. By day ten, it becomes completely embedded within the endometrium.
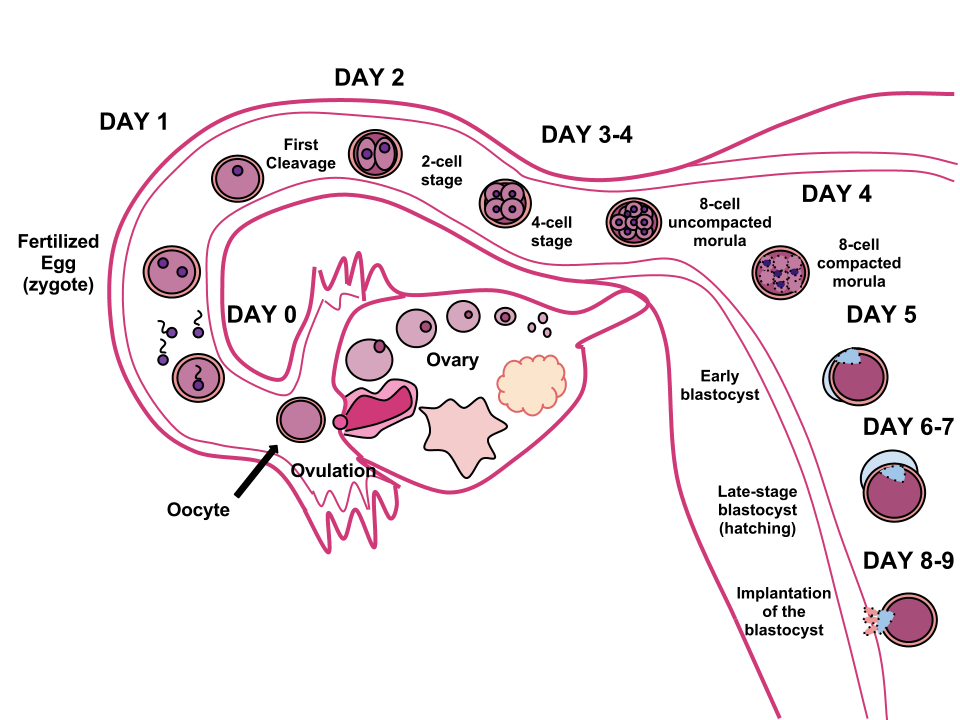
Courtesy of Ttrue12 CC BY-SA 3.0
Trophoblast Differentiation
The outer layer of the blastocyst, the trophectoderm, develops into trophoblast cells, which begin to differentiate by day eight. Two layers emerge: the cytotrophoblast, a mononuclear inner layer, and the syncytiotrophoblast, a multinucleated outer layer that invades the endometrial stroma and secretes human chorionic gonadotropin (hCG) to maintain progesterone secretion.
Trophoblast cells further specialise into villous and extravillous types. Villous trophoblasts form chorionic villi, which mediate oxygen and nutrient exchange, while extravillous trophoblasts migrate deeper into the uterine wall and maternal vasculature, establishing maternal–foetal blood flow by transforming spiral arteries.
The Yolk Sac and Early Circulation
The yolk sac appears around three weeks into gestation and is lined by extraembryonic endoderm. Although it does not contribute significantly to nutrition in humans, it plays a key role in early haematopoiesis. Blood is supplied via the primitive aorta and returned through vitelline veins, creating a circulatory loop known as the vitelline circulation.
By the end of the fourth week, the yolk sac becomes a small vesicle attached to the embryo by the vitelline duct, with part of it incorporated into the gut tube. The allantois, another structure derived from the yolk sac, contributes to the formation of the umbilical cord by giving rise to the umbilical arteries within the body stalk.
The Decidua
As pregnancy progresses, the maternal endometrium undergoes a process called decidualisation, under the influence of progesterone. The result is the formation of the decidua, which nourishes the embryo before placental circulation is fully established.
The decidua basalis lies beneath the implanted embryo and contributes to placental development. The decidua capsularis covers the embryo on the uterine side, while the decidua parietalis lines the rest of the uterus. By the fourth month, the decidua capsularis and parietalis fuse as the expanding amniotic cavity fills the uterus.
Amnion and Amniotic Fluid
The amnion begins as a thin membrane formed from ectodermal cells and eventually expands to enclose the embryo in a fluid-filled sac. Initially, amniotic fluid is an ultrafiltrate of maternal plasma. As the foetus matures, its own urine contributes to the fluid, especially from week 12 onward when renal function develops.
Amniotic fluid cushions the foetus, allowing for musculoskeletal development and protection from trauma. The amnion itself is a tough membrane, contributing significantly to the strength of the foetal membranes despite lacking nerves, blood vessels, or lymphatics.
Chorion and Chorionic Villi
The chorion is the outermost foetal membrane and is derived from the yolk sac. It forms chorionic villi, which are finger-like projections that invade the uterine lining to facilitate maternal–foetal exchange.
These villi develop in stages:
- Primary villi appear by days 13–15 as solid trophoblast outgrowths
- Secondary villi form when mesodermal tissue invades the core
- Tertiary villi develop by day 22 when chorionic blood vessels appear, establishing the foetal–placental circulation
Anchoring villi help secure the placenta by attaching the chorionic plate to the maternal decidua.
The Embryonic Period
The embryonic period spans from weeks 3 to 8 post-fertilisation and is the critical phase for organogenesis. By week 3, chorionic villi contain foetal blood vessels. By week 4, the basic foetal circulation and the primitive heart are functioning. Limb buds form, and by week 6, fingers, toes, and external ear structures are present.
The Foetal Period
From week 10 after the LMP onwards, the foetal period begins. This stage is characterised by growth and maturation of the organ systems formed during the embryonic phase.
By week 12, the foetus has developed peristalsis, the ability to swallow, and glucose transport begins. Ossification centres appear in bones, and external genitalia become distinguishable. Skin, nails, and hair also begin to form.
Between weeks 20 and 24, critical neurodevelopmental events occur. Neuronal proliferation and migration are largely complete, while neuronal organisation accelerates. Although the respiratory tree is well developed by this stage, the terminal alveoli are generally not yet formed, meaning that survival outside the uterus remains unlikely at 24 weeks without intensive neonatal support.
Header image used on licence from Shutterstock
Thank you to the joint editorial team of www.mrcgpexamprep.co.uk for this article.