Test your knowledge of central nervous system anatomy with these questions.
1. Which of the following cranial nerves originates in the midbrain?
A. Trochlear nerve
B. Trigeminal nerve
C. Vestibulocochlear nerve
D. Abducens nerve
E. Accessory nerve
Show Answer
Answer: A. Trochlear nerve
There are twelve paired cranial nerves in total and they all arise directly from the brain.
The cranial nerves are accordingly numbered by the location within the brainstem, (superior to inferior then medial to lateral), and the order of their exit from the cranium (anterior to posterior).
The first two cranial nerves, the olfactory nerve and the optic nerve, arise from the cerebrum, whereas the remaining ten cranial nerves arise from the brainstem. They either arise from a specific part of the brainstem (midbrain, pons, or medulla), or from a junction between the two parts.
Cranial nerves III-XII arise from the following locations within the brainstem:
| Location arisen from | Cranial nerve |
|---|---|
| Midbrain | Trochlear nerve (CN IV) |
| Midbrain-pontine junction | Oculomotor nerve (CN III) |
| Pons | Trigeminal nerve (CN V) |
| Pontine-medulla junction | Abducens nerve (CN VI) Facial nerve (VII) Vestibulocochlear nerve (CN VIII) |
| Medulla oblongata (posterior to the olive) | Glossopharyngeal nerve (CN IX) Vagus nerve (CN X) Accessory nerve (CN XI) |
| Medulla oblongata (anterior to the olive) | Hypoglossal nerve (CN XII) |
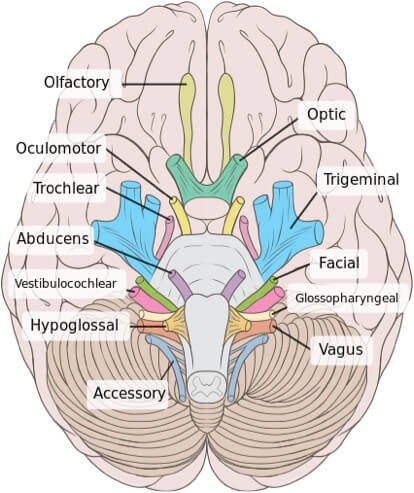
Image sourced from Wikipedia
Courtesy of Patrick J. Lynch CC BY-SA 2.5
2. At which anatomical location does the mandibular branch of the trigeminal nerve exit the skull?
A. Superior orbital fissure
B. Foramen rotundum
C. Internal auditory canal
D. Foramen ovale
E. Hypoglossal canal
Show Answer
Answer: D. Foramen ovale
The cranial nerves exit the skull at the following anatomical locations:
| Anatomical location | Nerve |
|---|---|
| Cribiform plate | Olfactory nerve (CN I) |
| Optic foramen | Optic nerve (CN II) |
| Superior orbital fissure | Oculomotor nerve (CN III) Trochlear nerve (CN IV) Trigeminal nerve (CN V1 – Ophthalmic nerve) Abducens nerve (CN VI) |
| Foramen rotundum | Trigeminal nerve (CN V2 – Maxillary nerve) |
| Foramen ovale | Trigeminal nerve (CN V3 – Mandibular nerve) |
| Internal auditory canal | Facial nerve (CN VII) Vestibulocochlear nerve (CN VIII) |
| Jugular foramen | Glossopharyngeal nerve (CN IX) Vagus nerve (CN X) Accessory nerve (CN XI) |
| Hypoglossal canal | Hypoglossal nerve (CN XII) |
3. Which of the following cranial nerves is correctly paired with its lesion?
A. The oculomotor nerve: the eye appears to look ‘down and out’
B. The hypoglossal nerve: hypertrophy of the tongue muscles
C. The vagus nerve: high-pitched quality to the voice
D. The abducent nerve: the eye is unable to look medially
E. The trochlear nerve: the eye appears to look ‘down and out’
Show Answer
Answer: A. The oculomotor nerve: the eye appears to look ‘down and out’
Lesions of the cranial nerves are outlined below:
Olfactory nerve (I)
A lesion of the olfactory nerve results in reduced smell and taste (except to ammonia which is carried in the trigeminal nerve as it stimulates the pain fibres).
Optic nerve (II)
Optic nerve lesions are complex and the clinical manifestation depends on where they occur in the visual pathway. They cause a variety of defects including hemianopias, quadrantanopias, sectoral defects and scotomas.
Oculomotor nerve (III)
Oculomotor nerve lesions usually result in a fixed, dilated pupil that does not accommodate. An unopposed lateral rectus results in the eye appearing ‘down and out’.
Trochlear nerve (IV)
The trochlear nerve supplies the superior oblique muscle, which abducts, depresses and internally rotates the eye. Lesions cause vertical diplopia and patients commonly tilt or lean their heads to allow better alignment of the eyes to compensate.
Trigeminal nerve (V)
The trigeminal nerve forms three trunks, the ophthalmic, maxillary and mandibular divisions. Lesions cause reduced sensation over whichever branch is involved. The ophthalmic division is also responsible for the corneal reflex. The mandibular division also supplies motor fibres to the masseter, temporalis and pterigoids. Lesions of this division therefore also cause weakness of jaw clenching and side-to-side movement. If the lesion is a lower motor one, the jaw deviates to the side of the lesion.
Abducens nerve (VI)
The abducens nerve supplies the lateral rectus muscle, which is responsible for abducting the eye. A lesion here results in the patient being unable to look laterally. The unopposed action of the medical rectus results in the eye being deviated medially. This commonly causes diplopia.
Facial nerve (VII)
Facial nerve lesions cause weakness of the facial muscles. If the lesion is a lower motor neurone one (as in Bell’s palsy) the forehead is involved, but if it is an upper motor neurone lesion, the forehead is spared because of bilateral innveration.
Vestibulocochlear nerve (VIII)
Vestibulocochlear nerve lesions result in unilateral sensorineural deafness and tinnitus.
Glossopharyngeal nerve (IX)
The glossophryngeal nerve receives sensory fibres from the tonsils, pharynx, middle ear and posterior 1/3 of the tongue. It also receives visceral sensory fibres from the carotid sinus and carotid bodies. Its only motor fibre supplies the stylopharyngeus muscle. Bilateral lesions here cause a pseudobulbar palsy.
Vagus nerve (X)
The vagus nerve supplies motor fibres to the palate and vocal cords and sensory fibres to the external acoustic meatus. Lesions can cause asymmetrical movement of the palate, nasal regurgitation of food and a nasal quality to the voice.
Spinal accessory nerve (XI)
The spinal accessory nerve gives motor supply to the sternocleidomastoid and trapezius muscles. A lesion here causes weakness of these muscles.
Hypoglossal nerve (XII)
The hypoglossal nerve supplies motor fibres to the tongue and infrahyoid muscles. A lower motor lesion here causes fasciculation and wasting of the ipsilateral muscles of the tongue, and when the tongue is stuck out it deviates to the side of the lesion. With an upper motor lesion the tongue deviates away from the side of the lesion.
4. Which of the following is would you expect to find in the presence of a frontal lobe lesion?
A. Increased spontaneous facial expression
B. Emotional stability
C. Perseveration
D. Bitemporal hemianopia
E. Acalculia
Show Answer
Answer: C. Perseveration
The frontal lobes are integral to our problem solving, being spontaneous, memory, language, judgment, sexual and social behaviour.
Lesions, strokes or trauma to this area can cause a multitude of problems, including the following:
- Reduced spontaneous facial expression
- Expressive dysphasia due to injury at Broca’s area (This is located in the posterior inferior frontal gyrus and is supplied by the middle cerebral artery)
- Perseveration
- Emotional lability
- Changes in personality
- Difficulty problem solving
- Impulsivity and disinhibition
- Depression and anxiety
- Loss of flexibility in thinking
Receptive dysphasia is due to damage to Wernicke’s area in the brain. This is located in the posterior superior temporal gyrus of the dominant hemisphere.
5. Which of the following could you expect to find when examining a patient with a temporal lobe lesion?
A. Prosopagnosia (difficulty in recognizing faces)
B. Expressive dysphasia
C. Increased risk taking
D. Perseveration
E. Left-right disorientation
Show Answer
Answer: A. Prosopagnosia (difficulty in recognizing faces)
The temporal lobes are involved in a variety of functions including visual, auditory, memory and how we categorize objects.
A stroke, space-occupying lesion or trauma to this area can result in a number of problems including:
- Receptive dysphasia (this is due to damage to Wernicke’s area in the brain that is located in the posterior superior temporal gyrus of the dominant hemisphere.
- Difficulty recognizing faces (Prosopagnosia)
- Inability to categorize objects
- Auditory agnosia
- Impaired musical perception
For thousands more anatomy tutorials and questions visit: www.anatomyprep.co.uk
Header image used on licence from Shutterstock




excellent learning
Excellent 👌
Excellent learning
Good recall testing of earlier years of Medical School.
Excellent refreshment
Hello Sir/madam hope you are will fine, i’m student of BSC MLT medical lab tech…..in india’s university.
i wanna to improve my medical special lab knowledge and i appreciate for you are because every one can make improve them knowledge by your helping and web site, hope all the best.