In Part 3 of our ‘Upper Limb Nerve Lesions’ series we learnt about the median nerve and the most commonly occurring lesions associated with damage to it. We now move on to the ulnar nerve and it’s associated nerve lesions.
The ulnar nerve is a major branch of the brachial plexus that arises as a continuation of the medial cord. It contains nerve fibres from spinal roots C8 and T1 (and also occasionally carries fibres from C7). It innervates muscles in the anterior compartment of the forearm and in the hand and supplies sensory innervation to the medial side of the hand and the medial one and a half fingers.
Anatomy of the Ulnar Nerve
The ulnar nerve arises in the brachial plexus and then travels down the upper arm medial to the brachial artery. It leaves the anterior compartment by passing posteriorly through the medial intermuscular septum with the superior ulnar collateral artery.
It then lies between the intermuscular septum and the medial head of triceps passing posterior to the medial epicondyle before entering the forearm between the two heads of flexor carpi ulnaris. The ulnar nerve is easily palpable at the medial epicondyle and is vulnerable to injury at this point.
It then lies medial to the coronoid process of the ulna, passes deep to flexor carpi ulnaris and on flexor digitorum profundus, with the ulnar artery on its lateral side from 1/3 of the way down the forearm. In the forearm it gives off the following branches:
- Muscular branches of the ulnar nerve
- Palmar cutaneous branch
- Dorsal cutaneous branch
The ulnar nerve lies lateral to the tendon of flexor carpi ulnaris at the wrist and then passes superficial to the flexor retinaculum and enters the hand through the ulnar canal (Guyon’s canal).
After entering the hand it divides into the following terminal branches at the pisiform bone:
- Superficial terminal branch
- Deep terminal branch
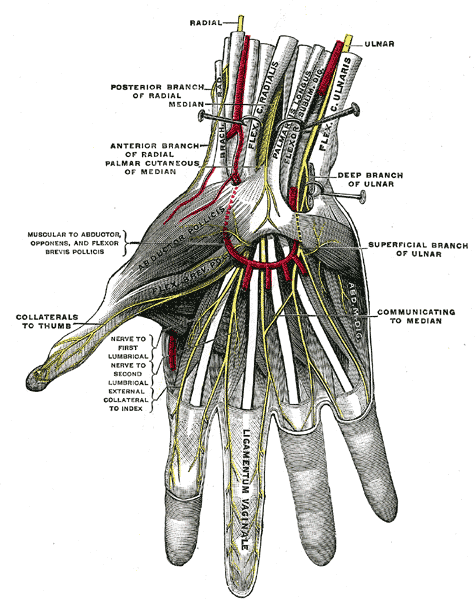
Fig 1. The superficial palmar nerves, showing the ulnar nerve and its branches in the hand (from Gray’s Anatomy).
The Motor Function of the Ulnar Nerve
The muscles supplied by the ulnar nerve and its two main motor branches are shown in the table below:
| Branch | Muscles supplied |
|---|---|
| Muscular branches of the ulnar nerve (in the forearm) | Flexor carpi ulnaris Flexor digitorum profundus (medial ½) |
| The deep branch of the ulnar nerve (in the hand) | Hypothenar muscles - Opponens digiti minimi - Abductor digiti minimi - Flexor digiti minimi brevis 3rd and 4th lumbricals Dorsal interossei Palmar interossei Adductor pollicis Flexor pollicis brevis (deep head) |
| The superficial branch of the ulnar nerve (in the hand) | Palmaris brevis |
The Sensory Function of the Ulnar Nerve
The sensory function of the ulnar nerve is provided by its three main sensory branches:
- Palmar cutaneous branch – supplies the medial half of the palm (arises in forearm and travels into the hand)
- Dorsal cutaneous branch – supplies the dorsal aspect of the medial 1 ½ digits and associated dorsal hand area (arises in forearm and travels into the hand)
- Superficial terminal branch – supplies the palmar aspect of the medial 1 ½ fingers (arises in the hand)
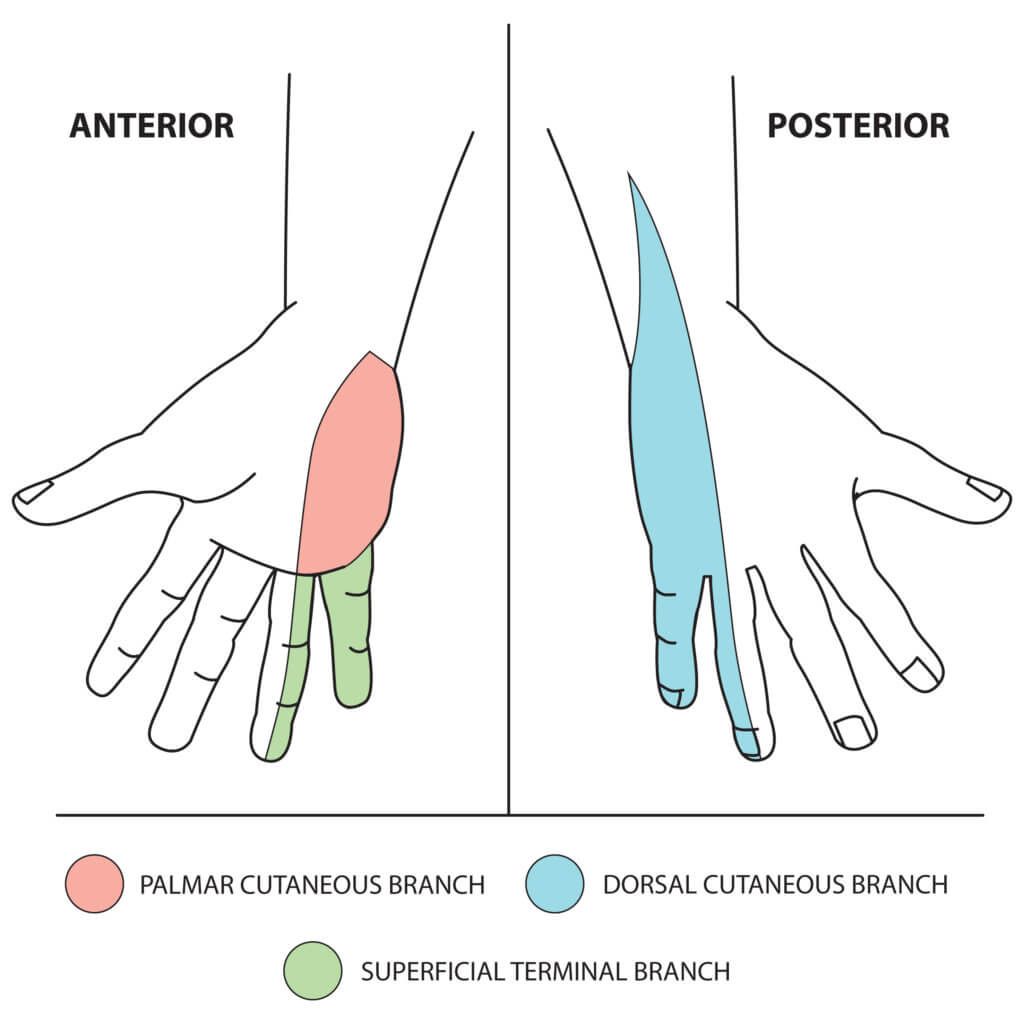
Fig 2. The sensory function of the ulnar nerve. © Medical Exam Prep
Ulnar Nerve Lesions at the Elbow
The ulnar nerve can be damaged by injury to or at the elbow. Fracture of the medial epicondyle, where the nerve is superficial and vulnerable, is the commonest mechanism.
Motor damage:
The medial half of flexor digitorum profundus and flexor carpi ulnaris will be paralysed. Flexion of the wrist can still occur (due to an intact median nerve) but will be accompanied by abduction (as flexor carpi ulnaris adducts the hand). There will be loss of all intrinsic muscles of the hand except lateral 2 lumbricals. Abduction and adduction of the fingers is lost and movement of the little and ring fingers is greatly reduced due to paralysis of the medial 2 lumbricals. The ‘claw hand’ appearance develops and Froment’s sign will be positive (see below). There is LESS clawing of little and ring fingers than when injured at the wrist (due to loss of flexor digitorum profundus).
Sensory damage:
All three cutaneous branches will be affected and there will be complete sensory loss in the areas that are innervated by the ulnar nerve.
Ulnar Nerve Lesions at the Wrist
The ulnar nerve can is most commonly damaged at the wrist by lacerations.
Motor damage:
Flexor carpi ulnaris and the medial half of flexor digitorum profundus, will be spared if the ulnar nerve is injured at the wrist. There will be loss of all intrinsic muscles of the hand except lateral 2 lumbricals. Abduction and adduction of the fingers is lost and movement of the little and ring fingers is greatly reduced due to paralysis of the medial 2 lumbricals. The ‘claw hand’ appearance develops and Froment’s sign will be positive (see below). There is MORE clawing of little and ring fingers than when injured at the elbow (due to an intact flexor digitorum profundus).
Sensory damage:
Sensory loss when the ulnar nerve is damaged at the wrist is variable but the two branches that arise in the forearm can be spared.
The Ulnar Claw
Damage to the ulnar nerve at either the elbow or wrist results in a characteristic ‘ulnar claw’ or ‘claw hand’ appearance with hyperextension of the metacarpophalangeal joints and flexion of the distal and proximal interphalangeal joint of the little and ring fingers. When the ulnar nerve has been damaged at the elbow there will be less clawing of the little and ring fingers as there will also be loss of flexor digitorum profundus to these fingers.
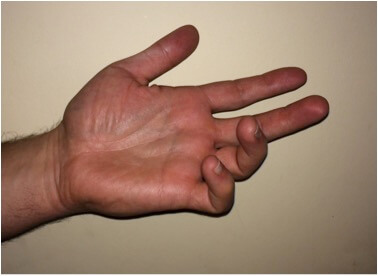
Fig 3. The ‘ulnar claw’.
Froment’s sign
Ulnar nerve lesions can be tested for by using Froment’s sign. This is tested for by placing a piece of paper between the patient’s thumb and index finger. The tester then attempts to pull the paper out of the patient’s pinched grip. In the case of an ulnar nerve palsy the patient will have difficulty maintaining the grip and will compensate by flexing flexor pollicis longus of the thumb to maintain grip pressure. The patient’s interphalangeal joint of the thumb will flex.
A comparison of ulnar nerve lesions at wrist and elbow is shown in the table below:
| Ulnar nerve at elbow | Ulnar nerve at wrist | |
|---|---|---|
| Motor loss | Wrist flexion accompanied by abduction Loss of all intrinsic muscles of the hand except lateral 2 lumbricals Loss of medial half of flexor digitorum profundus Loss of flexor carpi ulnaris | Normal wrist flexion Loss of all intrinsic muscles of the hand except lateral 2 lumbricals Flexor digitorum profundus and flexor carpi ulnaris both intact |
| Sensory loss | Loss of innervation to the anterior and posterior surfaces of the medial one and half fingers and the associated palm and dorsal hand area. | Loss of innervation to the palmar surface of the medial 1 and ½ fingers. Palmar and dorsal cutaneous branches may be spared. |
| Hand deformity | Claw hand deformity - LESS clawing of little and ring fingers due to loss of FDP | Claw hand deformity - MORE clawing of little and ring fingers due to intact FDP |
Thank you to the joint editorial team of www.anatomyprep.co.uk for this ‘Exam Tips’ blog post.
Header image used on licence from Shutterstock




wow i love it