A bundle branch block is a disorder in which there is an obstruction in the heart’s electrical conduction system. These can be broadly divided into two different types of block:
- Left bundle branch block (LBBB) – where the obstruction is in the left bundle branch
- Right bundle branch block (RBBB) – where the obstruction is in the right bundle branch
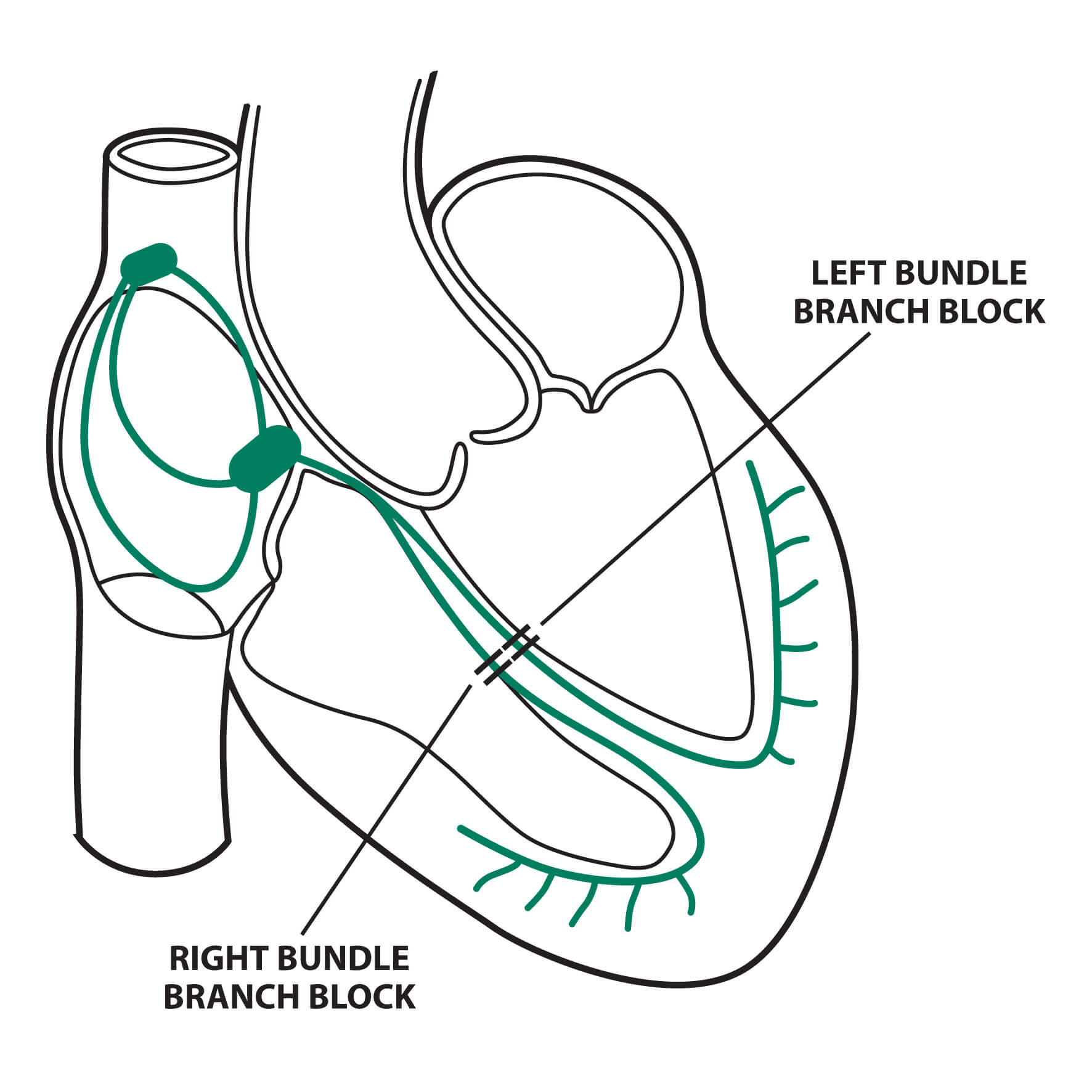
Fig 1. Anatomy of left and right bundle branch blocks © Medical Exam Prep
Left bundle branch blocks
In left bundle branch block (LBBB) the left ventricle is not directly activated by impulses travelling through the left bundle branch. The right ventricle, however, is still activated as normal by the right bundle branch.
The left ventricle is activated by impulses travelling through the myocardium across the septum. As this occurs more slowly than conduction through the bundle of His the QRS complex becomes widened.
Normally the septum is activated from left to right, which produces small Q waves in the lateral leads. In the presence of LBBB, however, this septal activation is reversed, which eliminates these normal septal Q waves.
The right to left depolarization of the myocardium produces deep S waves in the right praecordial leads (V1-V3) and tall R waves in the lateral leads (I, V5 and V6). It also usually causes left axis deviation. As the ventricles are activated sequentially from right to left, rather than simultaneously, the R wave in the lateral leads is broad and notched (‘M’ shaped)
Secondary T wave changes are a normal finding in LBBB. T wave changes are classed as secondary if the T wave is upright when the terminal portion of the QRS complex is negative and the T wave is inverted when the terminal portion of the QRS complex is positive. Primary T wave changes occur when these rules are violated and are consistent with myocardial ischaemia.
The diagnosis of ST-elevation myocardial infarction can be made in the presence of LBBB by using the Sgarbossa ECG algorithm.
The diagnostic criteria for LBBB are:
- Broad QRS complex (> 120 ms)
- Dominant S wave in lead V1
- Broad, monophasic R wave in lateral leads (I, AVL, V5 and V6)
- Prolonged R wave peak time > 60 ms in left praecordial leads (V5-V6)
- Absence of Q waves in lateral leads (I, V5 and V6)
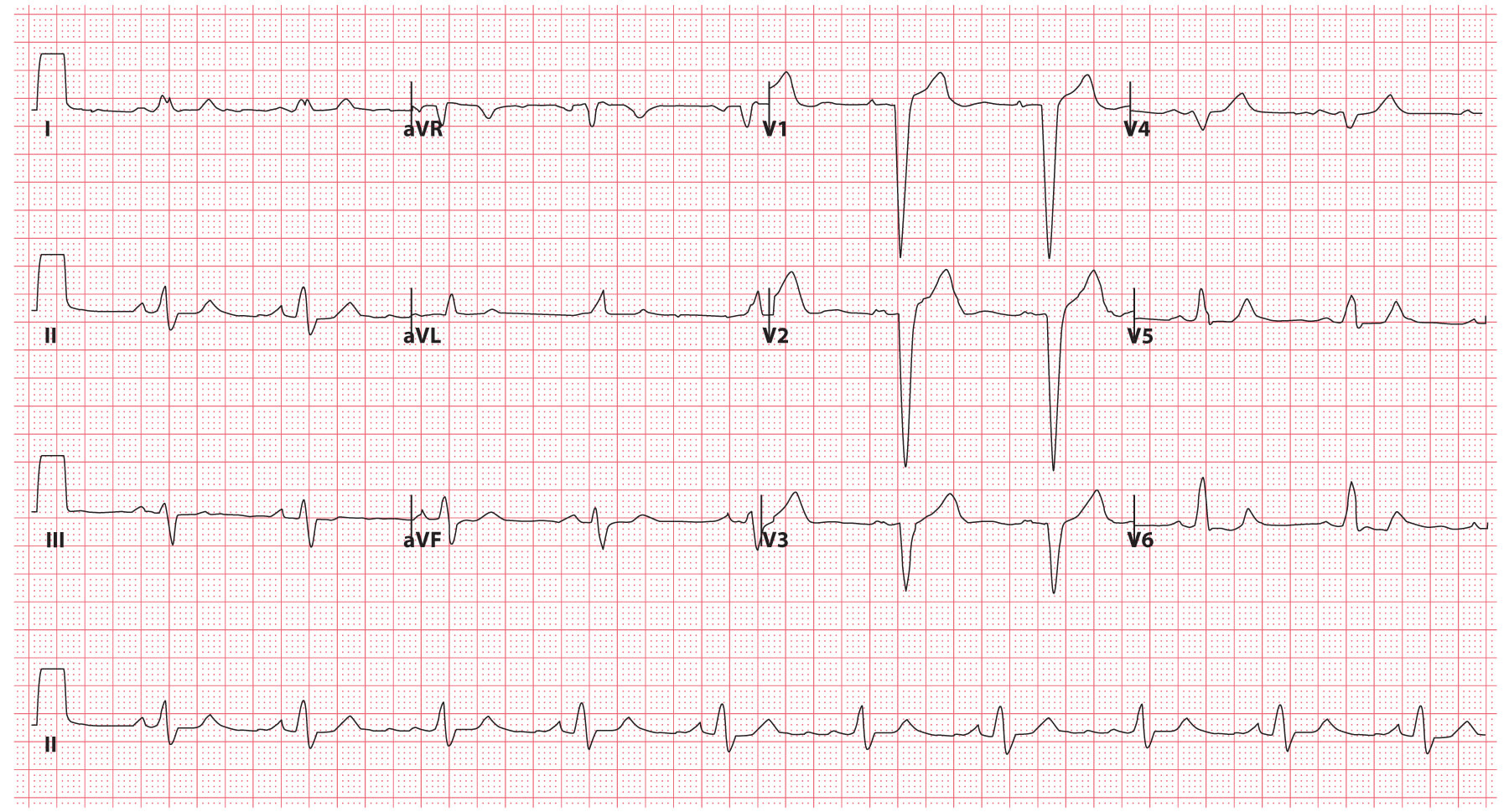
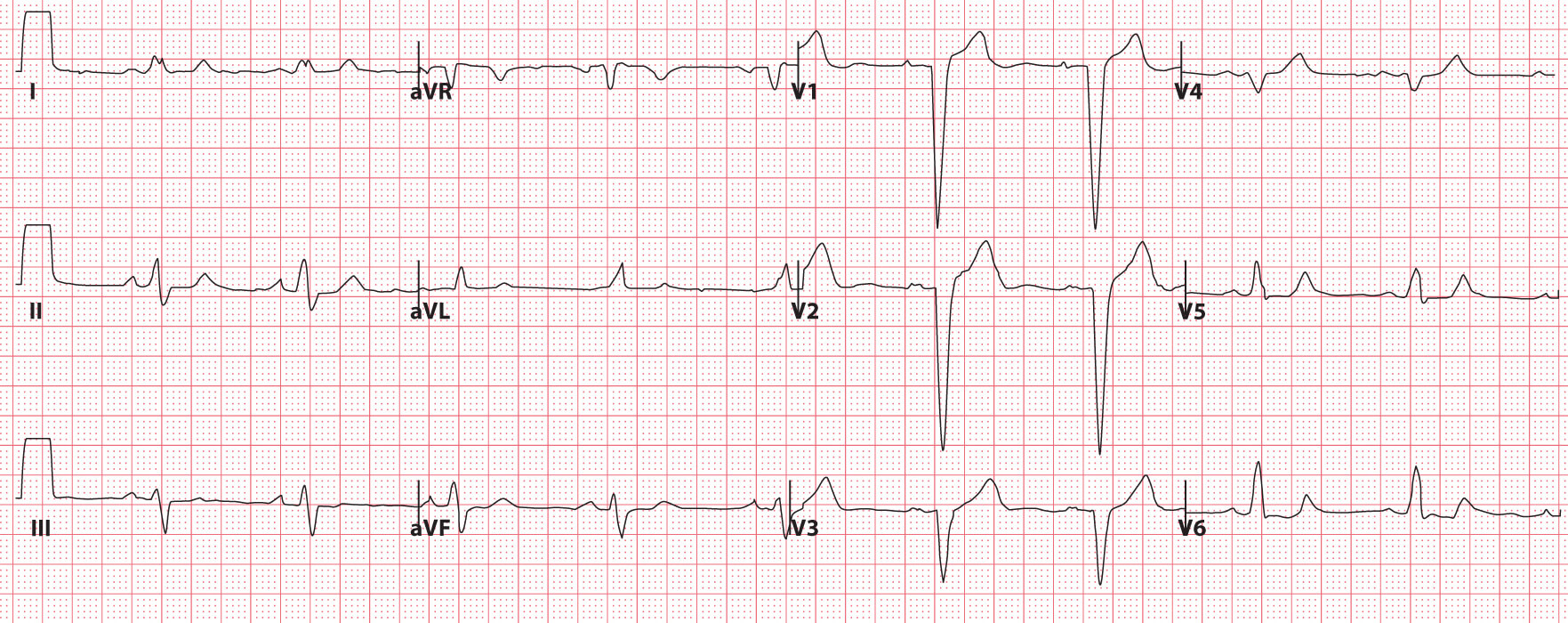
Fig 2. ECG example demonstrating LBBB © Medical Exam Prep
Right bundle branch blocks
In right bundle branch block (RBBB) the right ventricle is not directly activated by impulses travelling through the right bundle branch. The left ventricle, however, is still activated as normal by the left bundle branch.
The right ventricle is activated by impulses travelling through the myocardium across the septum. As this occurs more slowly than conduction through the bundle of His the QRS complex becomes widened.
As the left ventricle is activated normally the early part of the QRS complex remains unchanged. The delayed activation of the right ventricle, however, produces a secondary R wave (R’) in the right praecordial leads, and a wide, slurred S wave in the lateral leads. It also causes secondary repolarisation abnormalities, with T wave inversion and ST depression being seen in the right praecordial leads.
Secondary T wave changes are also a normal finding in RBBB. T wave changes are classed as secondary if the T wave is upright when the terminal portion of the QRS complex is negative and the T wave is inverted when the terminal portion of the QRS complex is positive. Primary T wave changes occur when these rules are violated and are consistent with myocardial ischaemia.
Unlike in the presence of LBBB, the changes of ST-elevation myocardial infarction can usually be clearly seen in RBBB.
The diagnostic criteria for RBBB are:
- Broad QRS complex (> 120 ms)
- RSR’ pattern in leads V1-V3 (‘M’ shaped QRS complex)
- Wide, slurred S wave in the lateral leads – I, AVL, V5 and V6 (‘W’ shaped QRS complex)
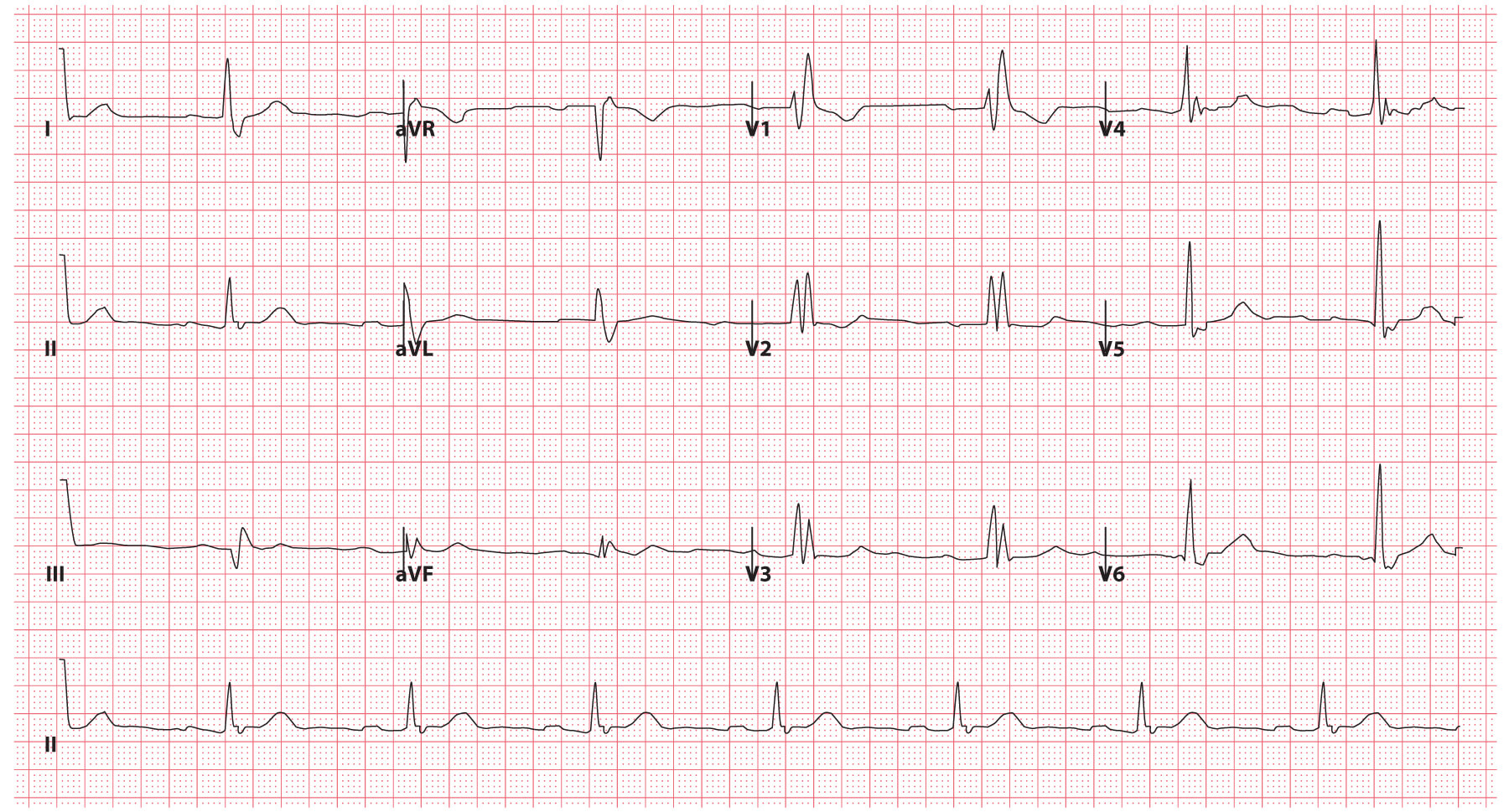
Fig 3. ECG example demonstrating RBBB © Medical Exam Prep
‘William Marrow’
A useful mnemonic for distinguishing between the ECG patterns of left bundle branch block (LBBB) and RBBB is ‘WiLLiaM MaRRoW’:
- WiLLiaM – in LBBB there is a ‘W’ in lead V1 and an ‘M’ wave in lead V6
- MaRRoW – in RBBB there is an ‘M’ wave in lead V1 and a ‘W’ wave in lead V6
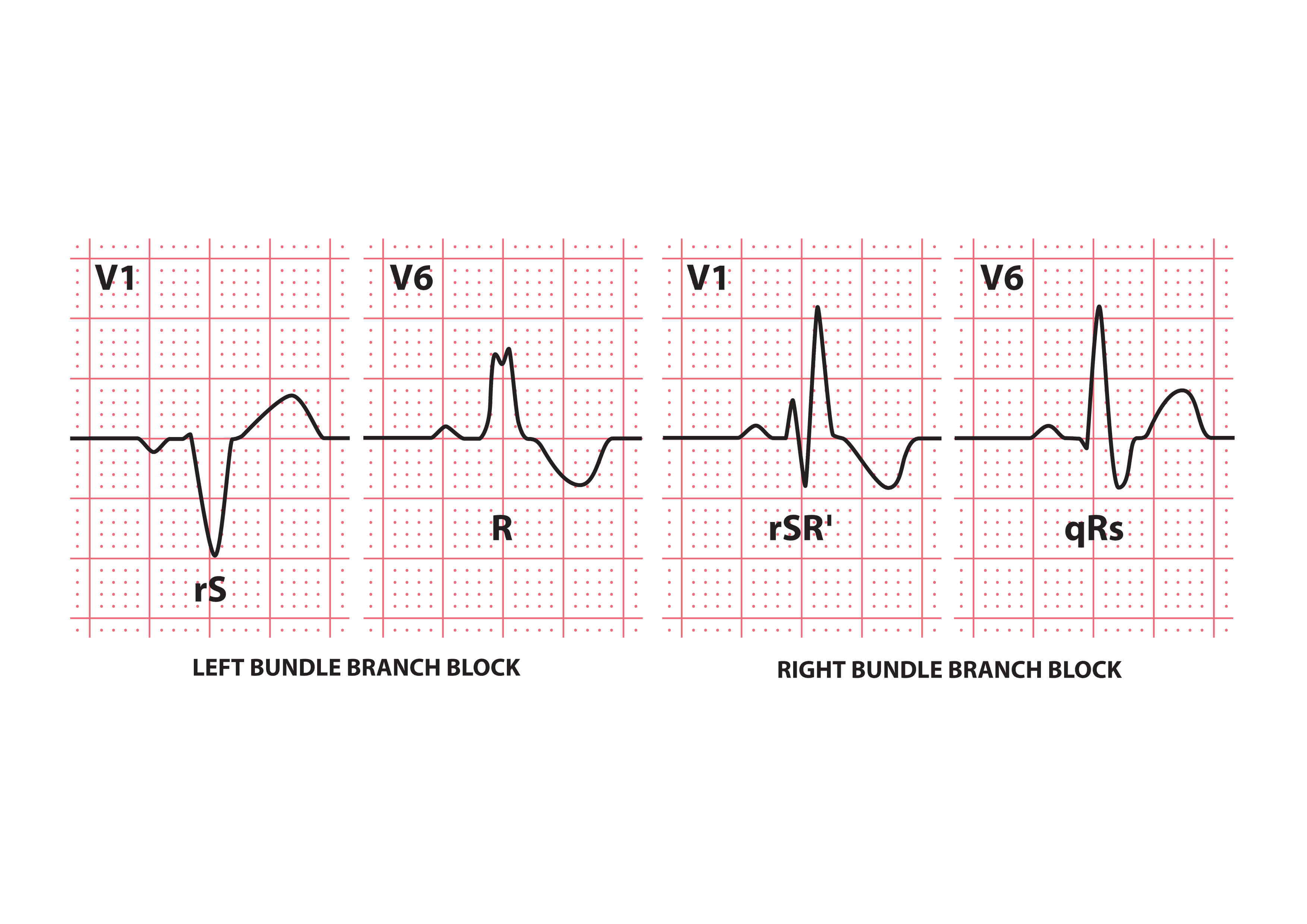
Fig 4. The characteristics of LBBB and RBBB © Medical Exam Prep
Causes of Bundle Branch Blocks
There are numerous potential causes of bundle branch blocks. RBBB can be a normal finding in young, healthy people. LBBB, unlike right bundle branch block, is almost always an indication of heart disease.
The commonest pathological causes are summarized in the table below:
| Left bundle branch block | Right bundle branch block |
|---|---|
| Ischaemic heart disease Anterior myocardial infarction Hypertension Aortic stenosis Dilated cardiomyopathy Primary fibrosis of the conducting system (Lenegre disease) Hyperkalaemia Digoxin toxicity | Ischaemic heart disease Rheumatic heart disease Right ventricular hypertrophy (cor pulmonale) Pulmonary embolus Cardiomyopathy Myocarditis Congenital heart disease (e.g. ASD) Degenerative disease of the conduction system |
Next: Bundle Branch Blocks (Part 2 – Fascicular Blocks)
Thank you to the joint editorial team of www.mrcemexamprep.net for this article.





Thank you!
Dealing with “All the Thorns under the skin”!
Thank you so much.