
In Part 1 of our ‘Bundle Branch Blocks’ series we learnt about left and right bundle branch blocks. Left bundle branch blocks can be further subclassified into left anterior fascicular blocks and left posterior fascicular blocks if the obstruction is limited to one fascicle only.
Under normal circumstances the left bundle branch consists of three fascicles:
- The left anterior fascicle, which supplies the upper and anterior parts of the left ventricle
- The left posterior fascicle, which supplies the posterior and infero-posterior parts of the left ventricle, and;
- The septal fascicle, which supplies the septal wall
Left Anterior Fascicular Block
In left anterior fascicular block (LAFB) the anterior portion of the left bundle branch is defective. In LAFB the cardiac impulses are therefore conducted to the left ventricle via the left posterior fascicle first, which creates a delay in the activation of the anterior and upper parts of the left ventricle.
The diagnostic criteria for LAFB are:
- Left axis deviation (axis usually between -45 and -90 degrees)
- Small Q waves with tall R waves in leads I and AVL (‘qR complexes)
- Small R waves with deep S waves in leads II, III and AVF (‘rS’ complexes)
- QRS duration normal or slightly prolonged (80-110 ms)
- Prolonged R wave peak time in AVL > 45 ms
- Increased QRS voltage in limb leads
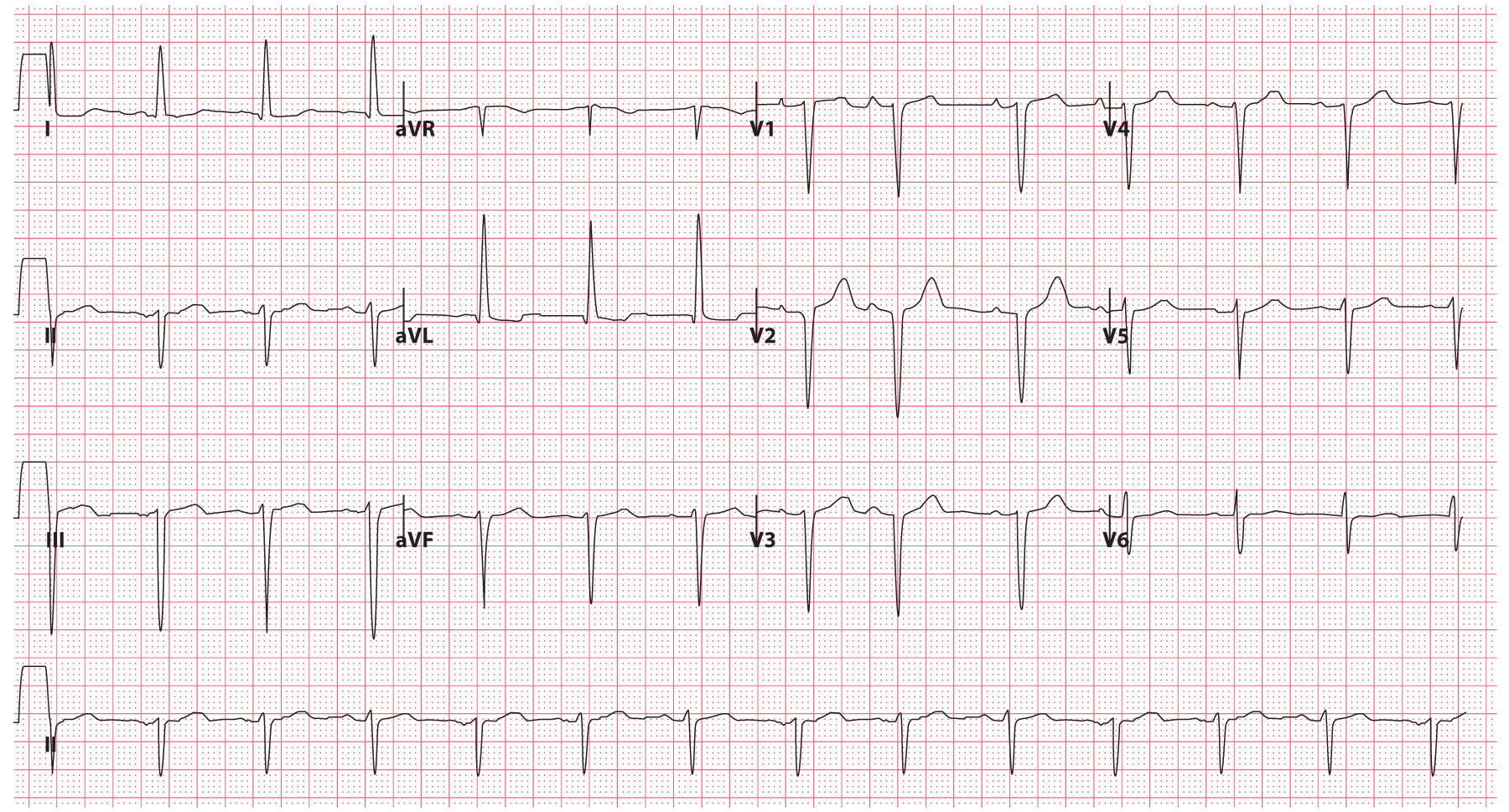
Fig 1. ECG example of LAFB © Medical Exam Prep
Left Posterior Fascicular Block
In left posterior fascicular block (LPFB) the posterior portion of the left bundle branch is defective. In LPFB the cardiac impulses are therefore conducted to the left ventricle via the left anterior fascicle first, which creates a delay in the activation of the posterior and infero-posterior parts of the left ventricle.
The diagnostic criteria for LPFB are:
- Right axis deviation (> +90 degrees)
- Small R waves with deep S waves in leads I and AVL (‘rS’ complexes)
- Small Q waves with tall R waves in leads II, III and AVF (‘qR’ complexes)
- QRS duration normal or slightly prolonged (80-110 ms)
- Prolonged R wave peak time in AVF > 45 ms
- Increased QRS voltage in limb leads
- No evidence of right ventricular hypertrophy
- No evidence of any other cause of right axis deviation
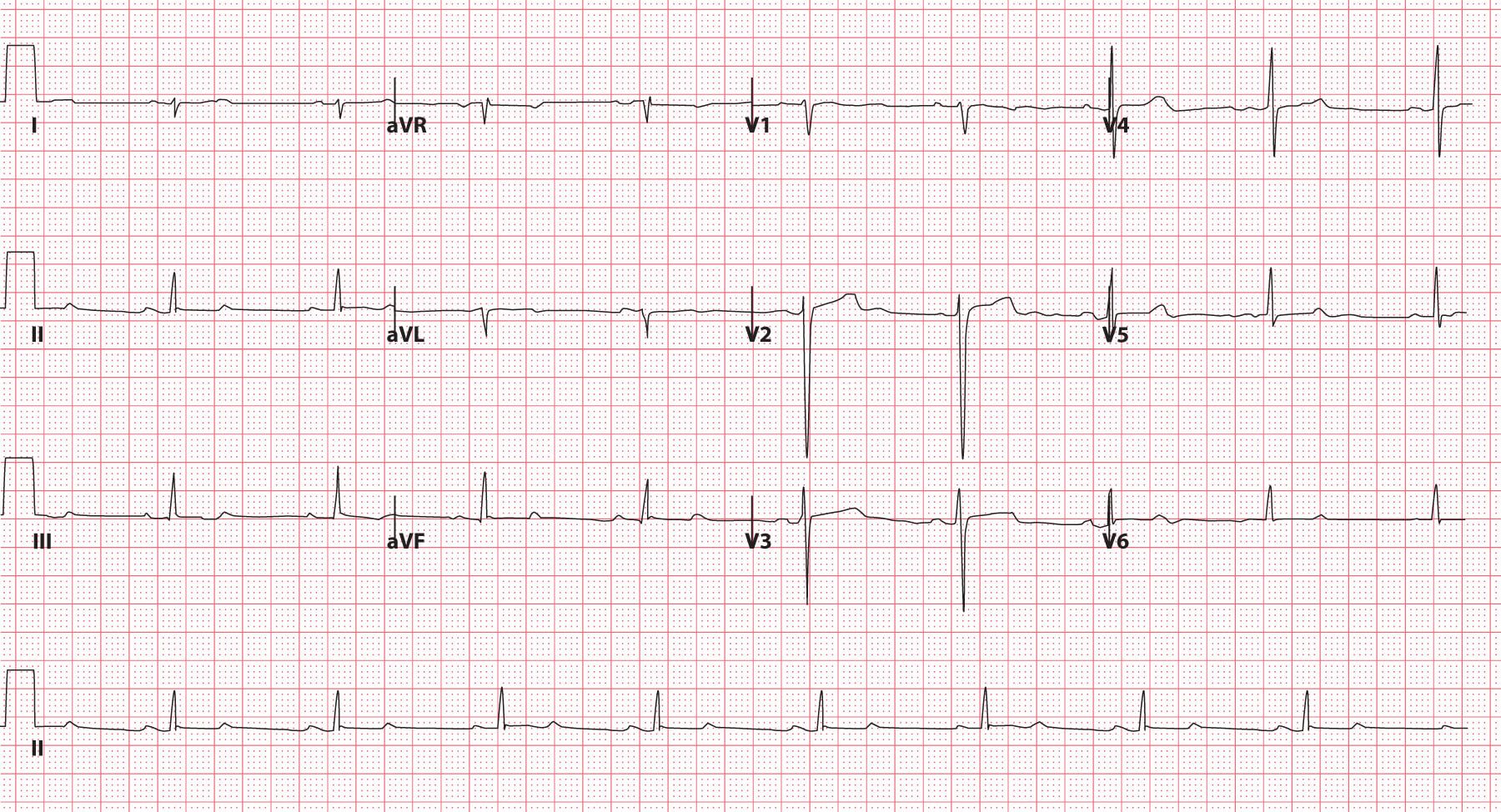
Fig 2. ECG example of LPFB © Medical Exam Prep
Bifascicular block
Bifascicular block is a conduction abnormality of the heart in which two of the three main fascicles of the His-Pukinje system are blocked.
This can be either:
- Right bundle branch block and left anterior fascicular block (most common pattern) or;
- Right bundle branch block and left posterior fascicular block
Although it is a sign of extensive conducting system disease, the risk of progression to complete heart block is relatively low (approximately 1% per year)
No treatment is usually required for asymptomatic patients but a pacemaker is recommended for those suffering syncope.
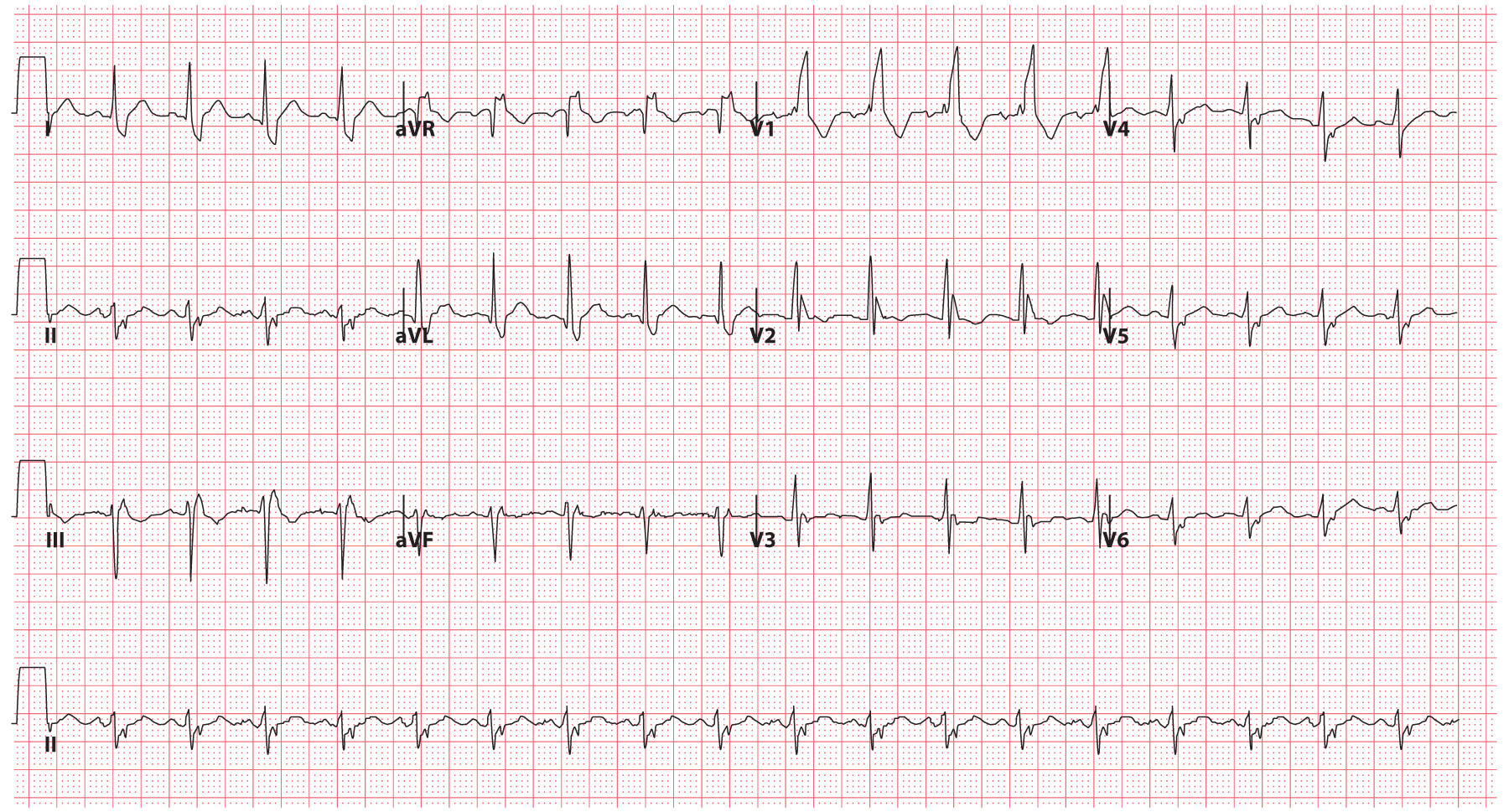
Fig 3. ECG example of bifascicular block (RBBB & LAFB) © Medical Exam Prep
Trifascicular block
Trifascicular block is a conduction abnormality of the heart in which two of the three main fascicles of the His-Pukinje system are blocked in combination with a first-degree atrioventicular (AV) block. The term ‘trifascicular block’ is something of a misnomer as the AV node is not a fascicle.
Trifasicular block can therefore be either:
- Right bundle branch block, left anterior fascicular block and first degree AV block, or;
- Right bundle branch block, left posterior fascicular block and first degree AV block
Trifascicular block is considered to be a precursor to complete heart block and it is estimated that there is a 50% lifetime need for the insertion of a permanent pacemaker in patients with trifascicular block.
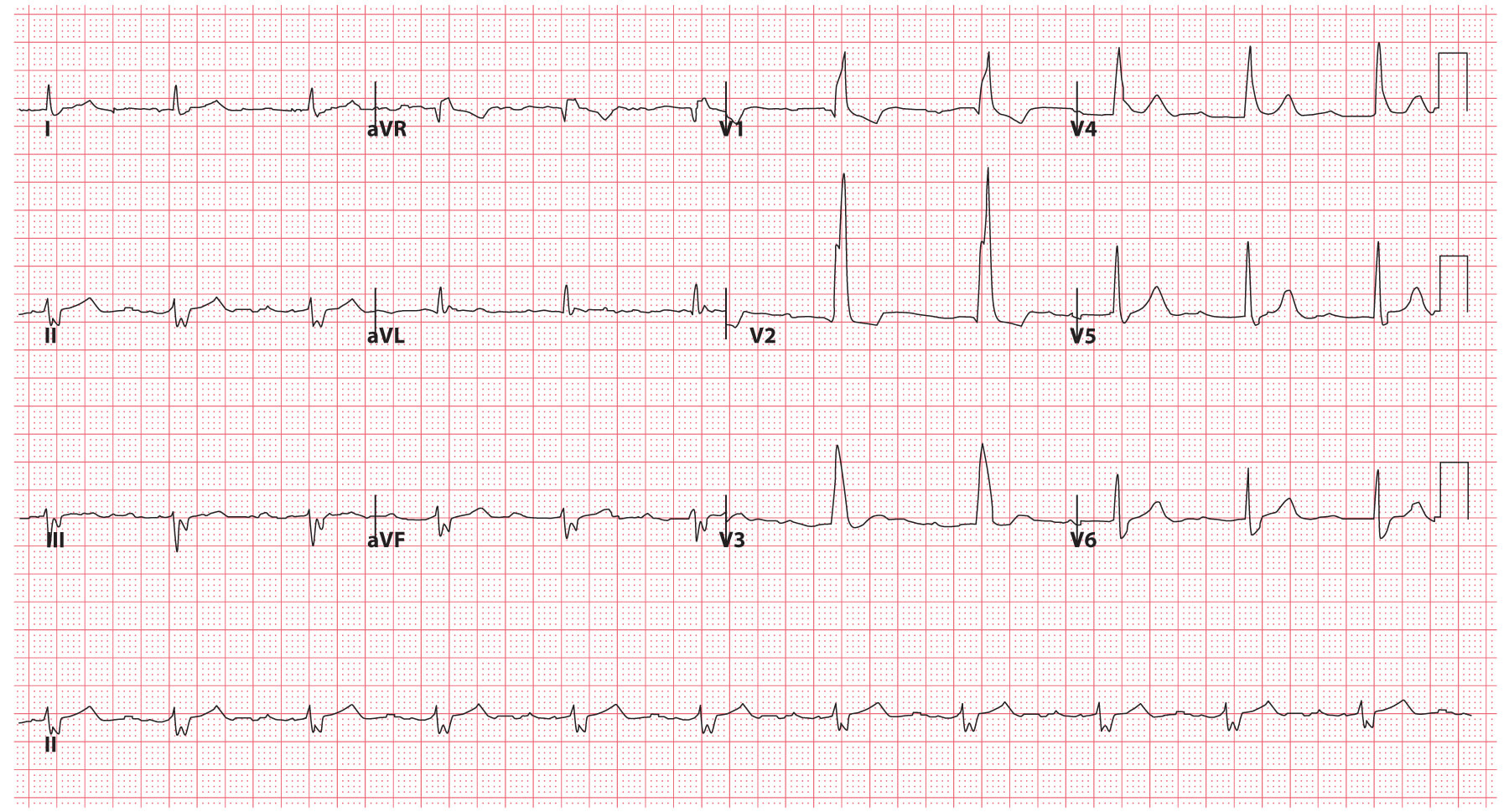
Fig 4. ECG example of trifascicular block (RBBB, LAFB and 1st degree AV block) © Medical Exam Prep
Thank you to the joint editorial team of www.mrcemexamprep.net for this article.




